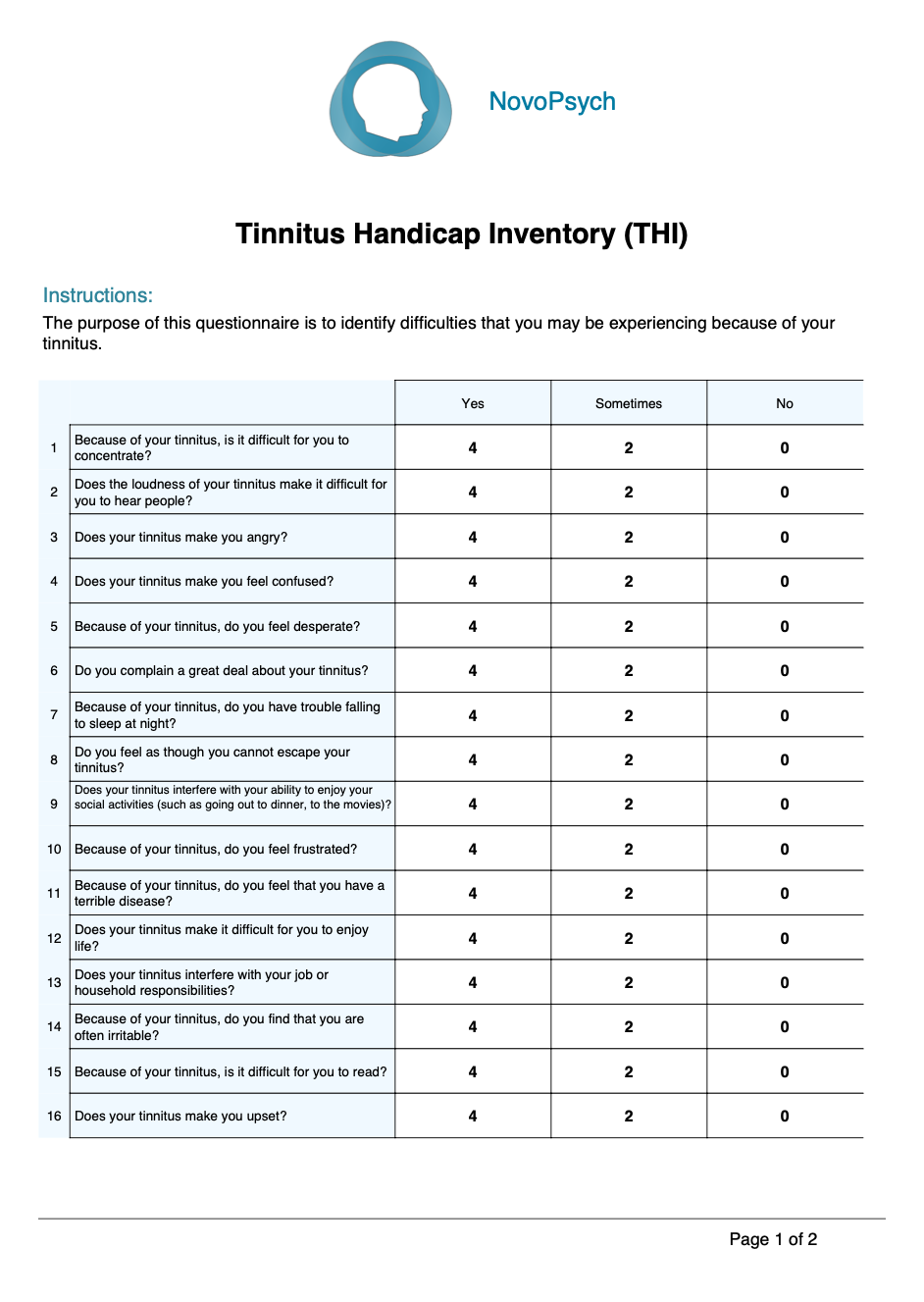
The THI comprises 25 items grouped into three subscales:
- Functional: this deals with limitations caused by tinnitus in the areas of mental, social, and physical functioning.
- Emotional: concerns affective responses to tinnitus, e.g. anger, frustration, depression, anxiety.
- Catastrophic: probes the most severe reactions to tinnitus, such as loss of control, inability to escape from tinnitus, and fear of having a terrible disease.
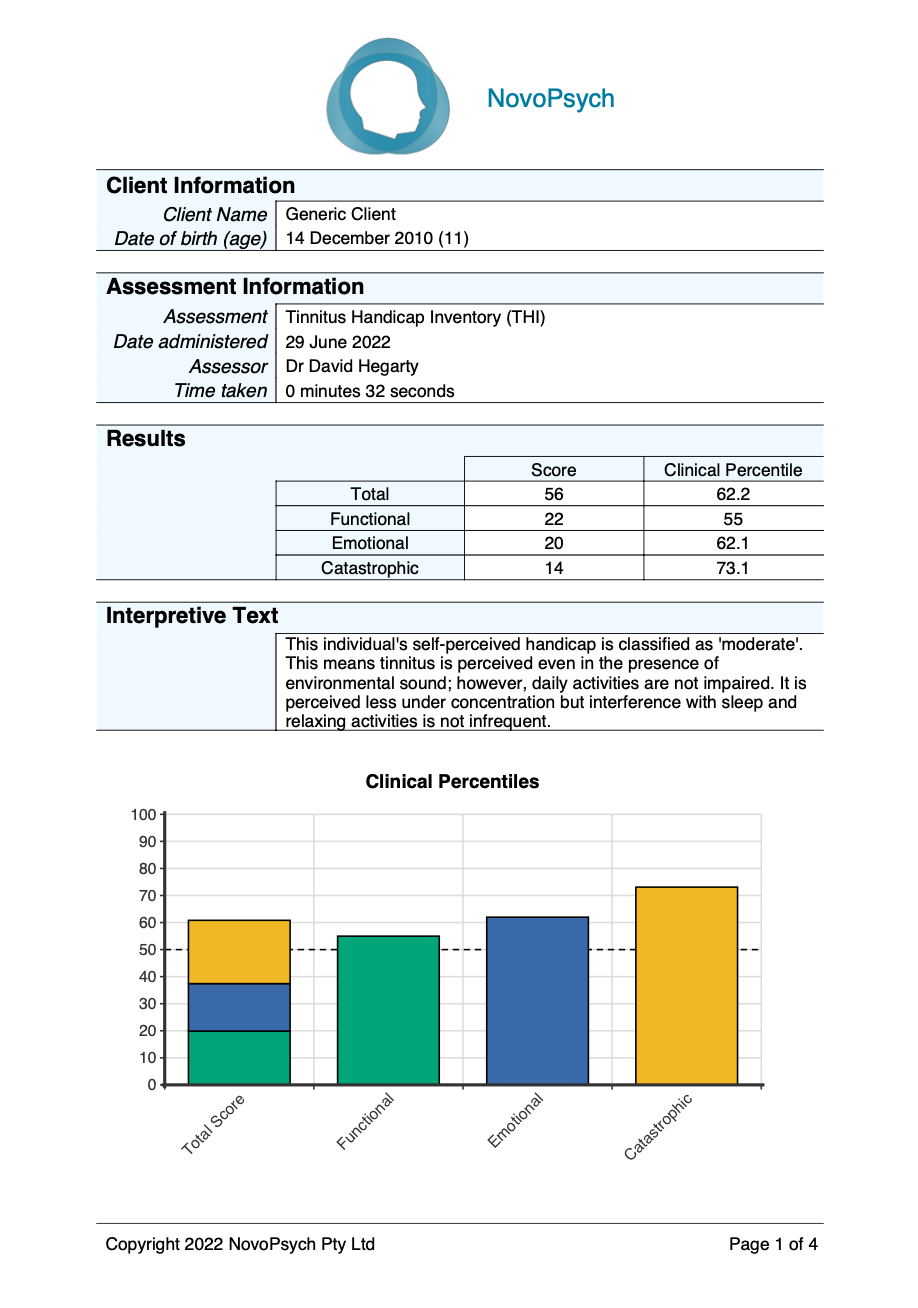
The THI total score ranges from 0 to 100 where a higher score indicates more tinnitus handicap severity. In addition, a percentile is presented that shows the respondents scores in comparison to tinnitus patients. A percentile rank of 50 indicates that the individual has an average severity of tinnitus compared to other people suffering tinnitus.
Three three subscales are calculated:
- Functional (items 1, 2, 4, 7, 9, 12, 13, 15, 18, 20, 24) – role limitations in the areas of mental, social/occupational, and physical functioning
- Emotional (items 3, 6, 10, 14, 16, 17, 21, 22, 25) – affective reactions to tinnitus
- Catastrophic (items 5, 8, 11, 19, 23) – catastrophic thinking about the symptoms of tinnitus, including a sense of lack of control
A grading system, as determined by the British Association of Otolaryngologists, Head and Neck Surgeons, is also used for the THI total score (McCombe et al., 2001):
- Very mild (score 0–16). Tinnitus is perceived only in silence and is easily masked. It does not interfere with sleep or with daily activities.
- Mild (score 18–36). Tinnitus is easily masked by environmental sounds and forgotten during daily activities. It can occasionally interfere with sleep but not with daily activities.
- Moderate (score 38–56). Tinnitus is perceived even in the presence of environmental sound; however, daily activities are not impaired. It is perceived less under concentration. Interference with sleep and relaxing activities is not infrequent.
- Severe (score 58–76). Tinnitus is continuously perceived and hardly masked by external noise. It alters the sleep cycle and can interfere with the subject’s daily activities. Relaxing activities are compromised. Subjects with this level of tinnitus often require medical consultations.
- Catastrophic (78–90). All side effects caused by tinnitus are present at a very severe level. The subject requires medical assistance very frequently, including neuropsychiatric help.
A change score of at least seven points has been considered to denote reliable clinically significant improvement on the THI (Zeman et al., 2011).
Studies concerning psychometric properties of THI report Cronbach’s alpha for the total score as very high, mostly above 0.90 (Gos et al., 2020). Alpha for the Functional and Emotional subscales ranged from 0.8 to 0.9, while for the Catastrophic subscale it was lower, about 0.6–0.7 (Gos et al., 2020). Although all three subscale scores are frequently used and reported, emphasis should be placed upon the total score (Gos et al., 2020).
In a validation study by Got et al. (2020), 1115 adult patients presenting at a tinnitus clinic (49.8% females, age range = 19 – 84; period of suffering tinnitus = 1 month – 50 years) were assessed using the THI and means (and standard deviations) were obtained:
- Functional: Mean = 20.53 (11.71)
- Emotional: Mean = 16.84 (10.30)
- Catastrophic: Mean = 10.81 (5.17)
- Total Score: Mean = 48.18 (25.27)
These means and standard deviations are used to calculate percentiles for the THI total score and subscale scores.