There are four symptom-areas assessed by the RAADS-R:
With high prevalence of Autism in mental health settings and the fact that adults are being referred for diagnosis with increasing frequency, this instrument is a useful clinical tool to assist clinicians with diagnosis (Ritvo et al., 2011).
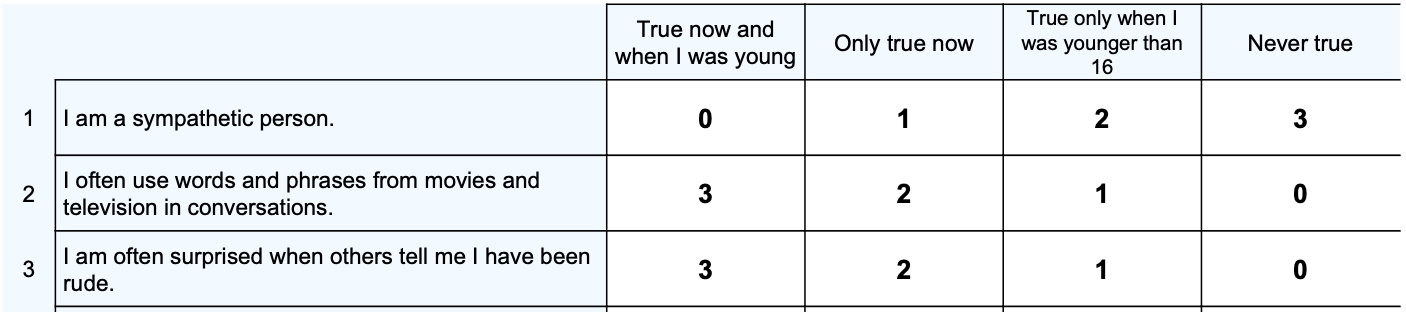
The RAADS-R is best used in conjunction with clinical expertise and/or other assessment procedures to establish a diagnosis. The self-report nature (with clinician supervision/administration) of this assessment may mean that individuals with low reflective capacity score low on the RAADS-R despite having diagnosable Autism.
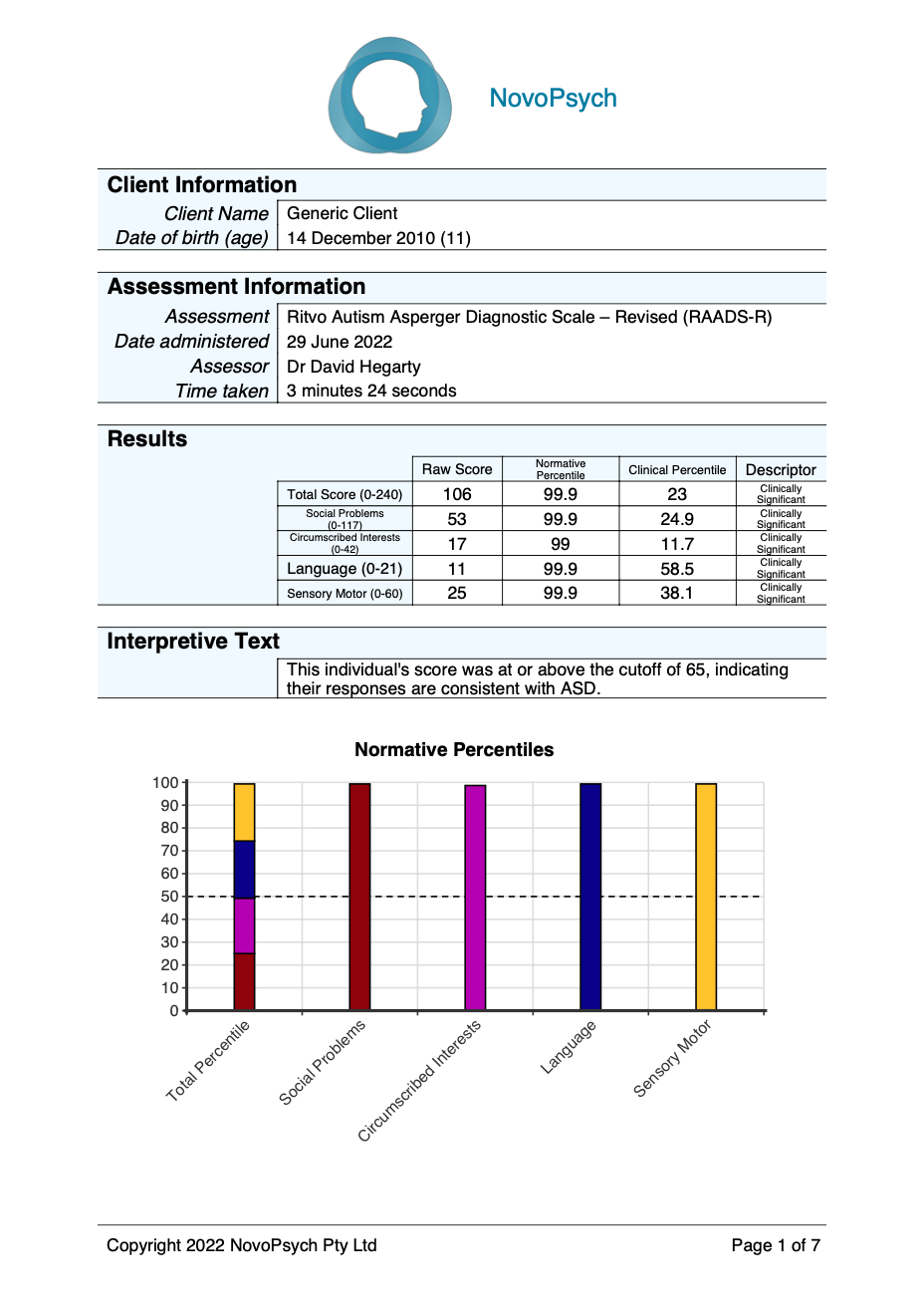
The total score of the RAADS-R ranges from 0 – 240, with a higher score more indicative of behaviours and symptoms consistent with Autism. Scores at or above 65 are consistent with Autism.
There is also a neurotypical and Autism percentile calculated that compares the respondent’s score with a comparison control group of neurotypical adults (Mean = 25.95, SD = 16.04) and adults with an Autism diagnosis (Mean = 133.81, SD = 37.72; Ritvo et al., 2011). The graph shows the respondent’s pattern of responding compared with the neurotypical sample, with the 50th percentile marking the average response for someone without Autism.
These percentiles can be helpful for interpretation as they contextualise scores in comparison to a typical pattern of responding for neurotypical adults and adults with Autism. For example, a normative percentile of 80 indicates the individual scored higher than 80 percent of the neurotypical comparison group. The cutoff raw score of 65 is above the 99th percentile on the neurotypical percentile, whereas this is at about the 3rd percentile for adults with Autism.
There are four subscales:
The self-report nature of this assessment may mean that individuals with low reflective capacity/insight score low on the RAADS-R despite having diagnosable Autism. It is therefore recommended that clinician’s inspect individual responses to items to judge the veracity of self-reported problems.
Questions on the original RAADS (Ritvo et al. 2008) assessed developmental pathology in three symptom areas: language, social relatedness, and sensory-motor. After critical review of the original RAADS and the results of a factor analysis, the revised 80-item RAADS-R was developed with the addition of a fourth symptom area (circumscribed interests), two questions, and several wording clarifications.
The RAADS–R is a valid and reliable instrument to assist the diagnosis of autistic adults. A validation study (Ritvo et al., 2011) with a sample of 201 adults with Autism and 578 neurotypical adults from the USA and Australia (Ritvo et al., 2011) defined the optimum cutoff score of 65. At this level, no one without Autism scored above the threshold (specificity = 100%) and only 3% of the autistic group did not score over the cutoff score (sensitivity = 97%). Test–retest reliability was high (0.987) and it had high concurrent validity (96%) with the SRS-A.
The Autism norms which are used to calculate Autistic percentiles are based on the validation study by Ritvo, et al. (2011). A sample of 201 individuals with a confirmed DSM-IV-TR diagnosis of Autism or Aspergers had a mean RAADS-R score of 133.81 (SD = 37.72). This combined Autism and Aspergers group had an average age of 31, IQ of 119 and were 28% female. The Autism group alone had a mean RAADS-R score of 138.46 (SD = 41.4), however the combined group was used in calculating percentiles given it is most representative of DSM-5-TR diagnostic criteria.
The neurotypical percentile is based on a sample of 578 individuals who did not have a diagnosis of Autism, Aspergers or PDD NOS, however did include people with other high prevalence clinical diagnoses, making it representative of a neurotypical population. The sample had an average age of 42, IQ of 114 and 57% percent were female. The normative sample’s mean RAADS-R score was 25.95 (SD = 16.04) and is used to calculate the normative percentile.