Past research has found that MDQ total scores are associated with anxiety, trauma-related, substance use, eating, and impulse control disorders, in addition to BD (Paterniti & Bisserbe, 2018; Zimmerman et al., 2011). As a result, there have been two subscales identified (Carpenter et al., 2020):
Research indicates that effective treatment of bipolar disorder (BD) differs significantly from that of other related disorders, such as unipolar depression (Carpenter et al., 2020). This underscores the importance of screening for bipolar disorder (BD) in patients who present to mental health services so that they can receive an effective intervention. For example, the use of antidepressants in BD treatment is controversial (Sidor & MacQueen, 2011) and psychotherapy treatment more often involves addressing issues such as unrealistic goal-setting and impulsivity in patients with BD than in others (Geddes & Miklowitz, 2013; Miklowitz & Johnson, 2006). As BD is associated robustly with significant psychosocial impairment (e.g., poor work and relationship functioning), failing to detect cases of BD can lead to suboptimal treatment approaches and, thereby, exacerbate personal and societal costs associated with BD (Conus, Macneil, & McGorry, 2014).
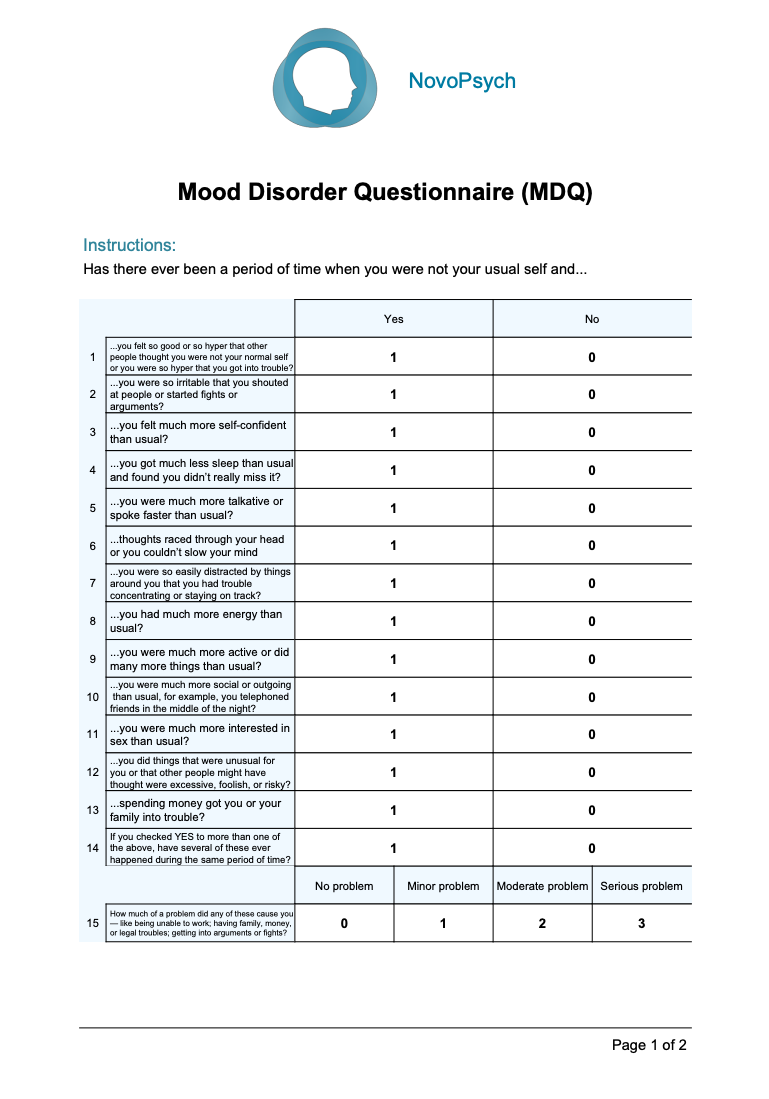
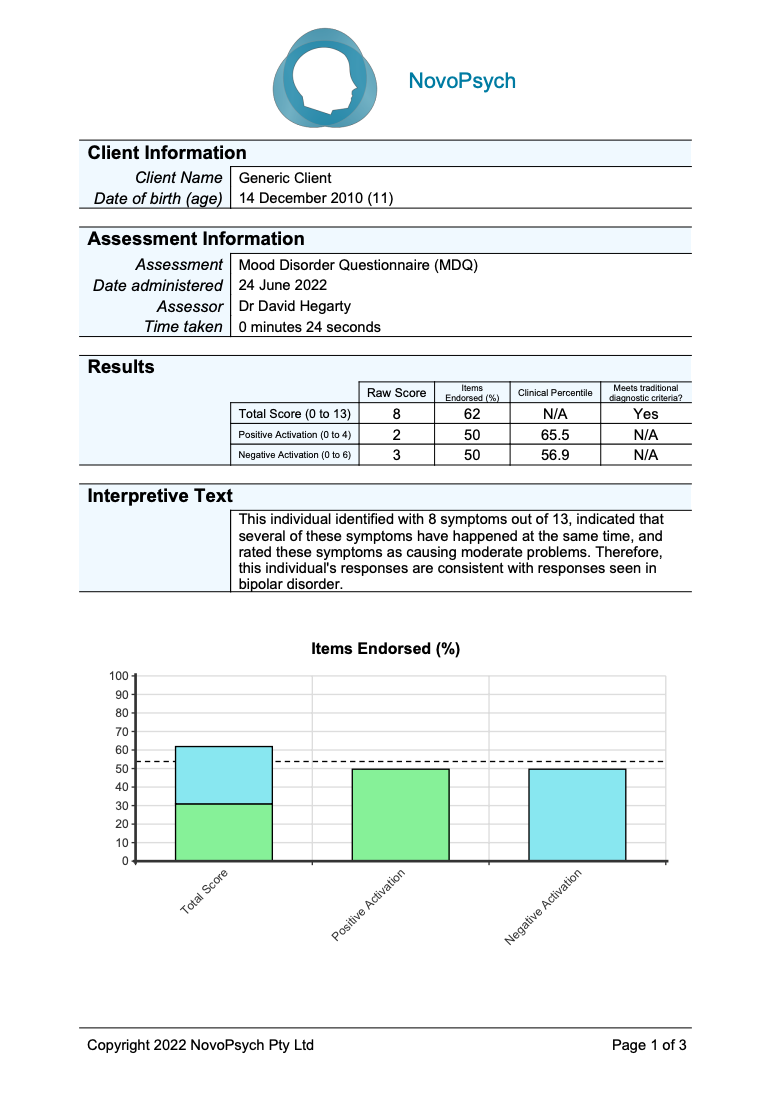
A total score is calculated for questions 1-13 where a “Yes” provides a score of 1 and “No” is 0. The percentage of items endorsed (raw score / number of items multiplied by 100) is included to provide an indication of the proportion of symptoms identified with by the respondent.
In order to meet the threshold for bipolar disorder the traditional scoring method is as follows:
Subscale scores were also developed (Carpenter et al., 2020, Stanton & Watson, 2017) using 10 of the 13 items in the symptom questions:
Clinical percentiles are also presented for the two subscales as developed by Carpenter et al. (2020) on over 1,700 outpatients (for a variety of diagnoses). A percentile of 50 means that the client has scored at the average level compared with the clinical group for that subscale.
The internal reliability for the MDQ is strong (Cronbach’s alpha = 0.88; Stanton & Watson, 2017).
Traditionally, a positive screen on the MDQ requires endorsement of (a) 7 or more of 13 symptom items, (b) multiple symptoms occurring at the same time, and (c) symptoms causing notable psychosocial impairment (Hirschfeld et al., 2000). The first thirteen questions on the MDQ are based upon bipolar symptoms and a score of 7 or more is the optimal cutoff, as it provides good sensitivity (73%) and very good specificity for a diagnosis of BD (90%; Hirschfeld et al., 2000). However, results from a number of studies suggest that the MDQ is not unidimensional (Ruggero et al., 2014; Stanton & Watson, 2017).
Carpenter et al. (2020) and Stanton and Watson (2017) investigated the structure of the MDQ’s 13 symptom items and found that the MDQ was best represented by two factors, which they termed Positive Activation (e.g., “had much more energy”; “was much more confident”) and Negative Activation (e.g., “thoughts raced”; “felt very irritable”) symptom dimensions. Three of the MDQ symptoms (items 5, 10, and 11) loaded highly onto both Positive and Negative Activation factors and were removed from the final model. Carpenter et al. (2020) found that Positive Activation was uniquely associated with BD diagnosis, whereas Negative Activation was associated with a range of diagnoses. Thus, a 4-item Positive Activation subscale (α = .82) and a 6-item Negative Activation subscale (α = .73) was created.