The RCADS-Child (Chorpita et al., 2000) consists of six subscales that screen for high prevalence disorders in youth:
In addition to the subscales, a Total Internalising score that is a combination of all six subscales is provided that gives an overall indication of the level of internalising problems. A Total Anxiety score that is a combination of the five anxiety subscales provides an overall indication of anxiety problems.
A parallel parent-report version, the RCADS-Parent, can be used in conjunction with the RCADS-Child to gather additional clinical information. The RCADS is well-suited for screening and monitoring of anxiety and depressive symptoms in youth.
Example RCADS-Child Items:
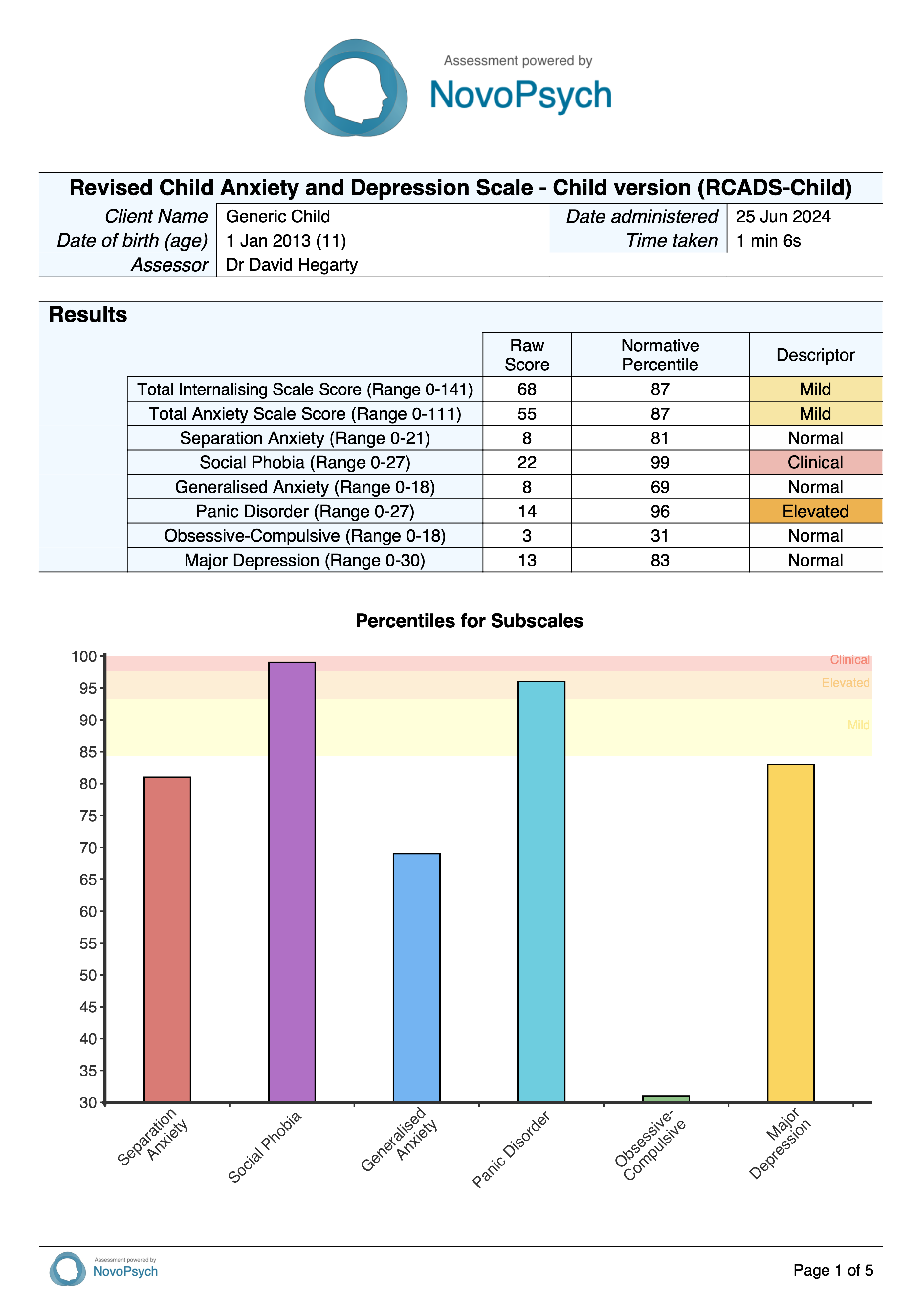
The RCADS-Child yields a Total Internalising Scale (sum of all 6 subscales) and a Total Anxiety Scale (sum of 5 anxiety subscales) to provide an overall indication of symptom severity. The RCADS provides raw scores for the six subscales that are converted to percentiles based on the child’s age group (8-12 or 13-18 years) from the Australian normative data. A percentile of 50 reflects the average symptom level relative to same-aged peers, while increasingly higher percentiles indicate more severe symptoms (e.g. > 93.31st percentile signifies elevated symptoms).
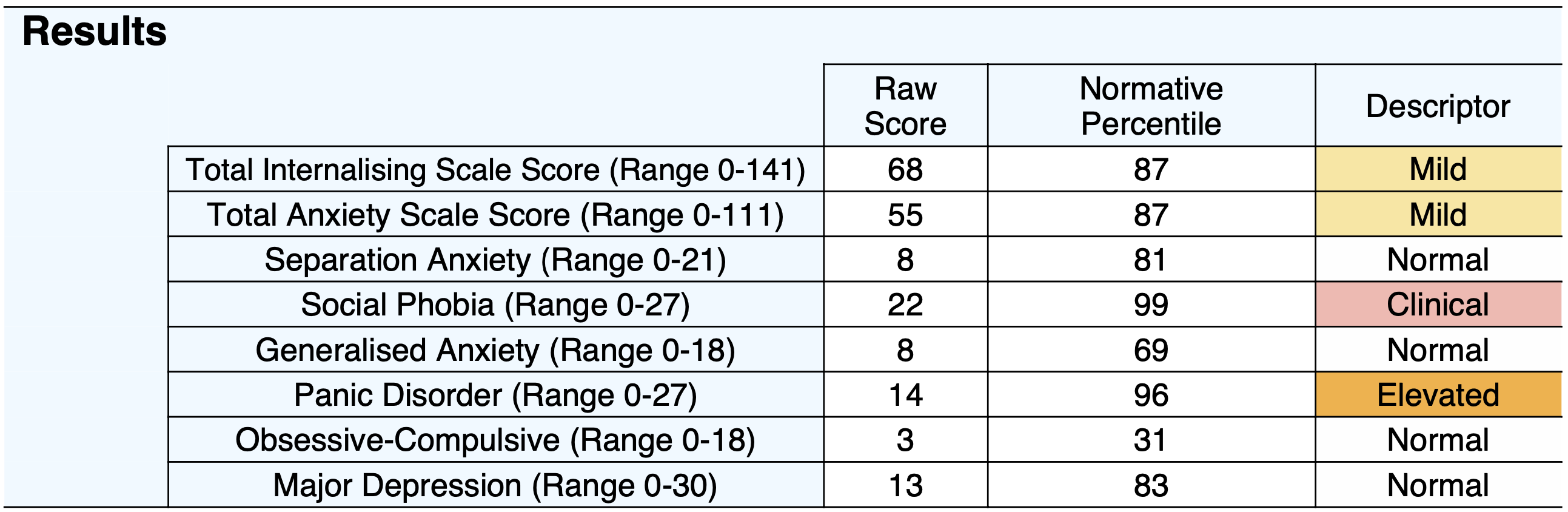
A descriptor is provided based upon the following criteria:
The six subscales assessed by the RCADS-Child are:
The RCADS subscales are best conceived as dimensional symptom clusters rather than diagnostic categories. Higher scores suggest greater symptom severity and clinical risk and should be integrated with clinical judgement to guide diagnostic formulation and treatment planning.
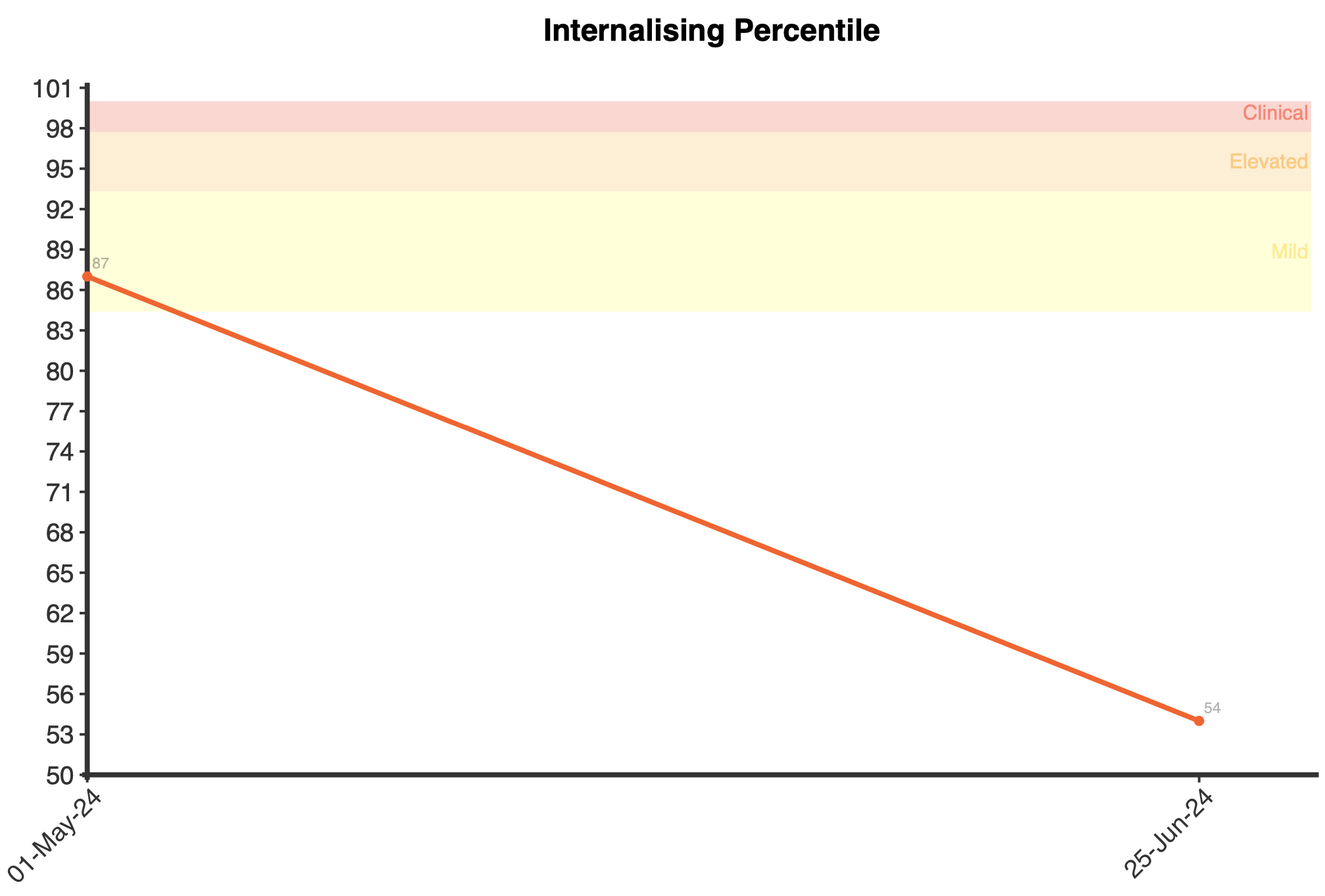
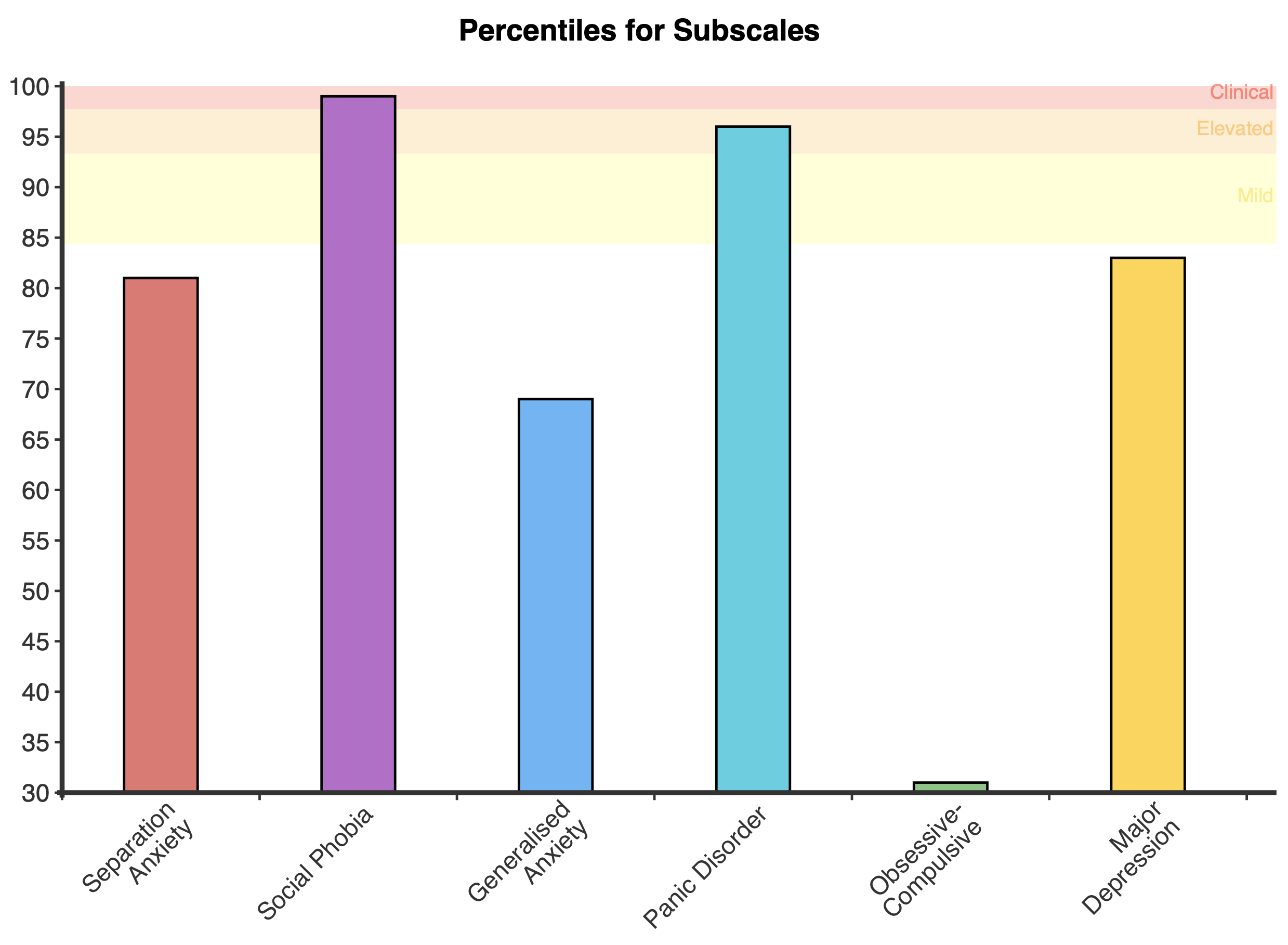
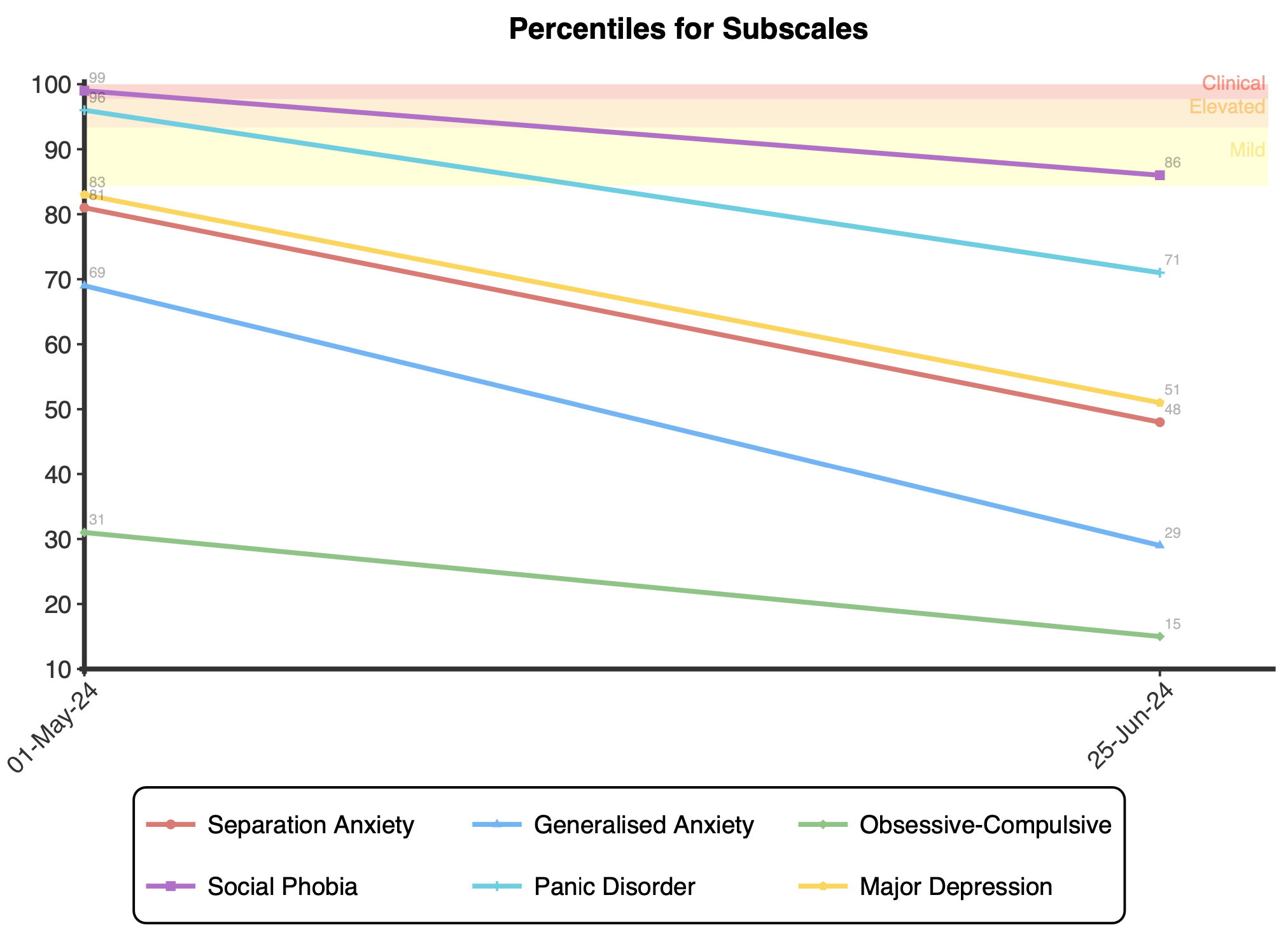
Plots demonstrating the subscale percentiles are presented upon first administration. Longitudinal plots are displayed for both the subscale percentiles and the Total Internalising and Anxiety percentiles upon multiple administrations to enable tracking of symptoms over time.
The RCADS was developed using anxiety items from the Spence Children’s Anxiety Scale (Spence, 1997) and adding a depression scale, then validated in a large community sample of children and adolescents (N = 1,641) by Chorpita et al. (2000). Exploratory factor analysis yielded a 6-factor solution consistent with DSM-IV anxiety and depressive disorders. The measure has demonstrated good internal consistency for all subscales (α = .71-.85) and the Total Internalising Scale (α = .93-.96). Test-retest reliability was also satisfactory over a 1-week interval (rs = .65-.80; Chorpita et al., 2000).
Confirmatory factor analysis in separate child and adolescent samples supported the 6-factor structure, with acceptable goodness-of-fit (Chorpita et al., 2005). The RCADS has shown good convergent and discriminant validity with other established measures of child anxiety and depression (Chorpita et al., 2005; Ebesutani et al., 2010, 2012).
The psychometric properties of the RCADS have been further examined in an Australian community sample of youth aged 8-18 (N = 405; de Ross et al., 2002). Results mirrored those of Chorpita et al. (2000), with the 6-factor model exhibiting satisfactory fit. The Australian sample was split into younger (8-12) and older (13-18) age groups to provide normative and percentile data for contextualising scores (if used with clients outside of this age range then percentiles are calculated using combined 8-18 years data).
The percentiles for the Total Internalising Score and the Total Anxiety Score were interpolated using the de Ross et al. (2002) data for subscale scores. This was done using percentile intervals of 5 (i.e., 5, 10, 15…) where the score for each subscale was calculated using subscale means and standard deviations and summed to provide an estimate of the combined score for each percentile interval. Percentiles between the intervals were then interpolated using a linear approach to determine corresponding percentiles for each possible score.
Descriptors are based upon T-Scores, however for ease of interpretation these scores are converted to percentiles:
Note the ‘Mild’ descriptor range was added by NovoPsych to be consistent with the interpretation of the Spence Children’s Anxiety Scale (Spence, 1997), from which the RCADS-Child was derived, where scores above the 84th percentile are classified as clinically significant anxiety symptoms.
A reliable change score has been determined by NovoPsych for the Internalising Score from data collected between July 2020 and June 2024 where clients had completed multiple RCADS-Child assessments. All data was included in the analysis, so no data was removed based upon initial symptom severity. The resultant sample size was 7,695. The reliable change score was calculated using the Jacobson-Truax method of clinical significance classification (Jacobson & Truax, 1991) using calculated Cronbach alpha’s from the NovoPsych data. The internal reliability calculated for the Internalising Score was 0.96 and the reliable change score calculated was 15.
For comprehensive information about the RCADS, see the RCADS website
The percentiles for the Total Internalising Score and the Total Anxiety Score were interpolated using the de Ross et al. (2002) data for subscale scores. This was done using percentile intervals of 5 (i.e., 5, 10, 15…) where the score for each subscale was calculated using subscale means and standard deviations and summed to provide an estimate of the combined score for each percentile interval. Percentiles between the intervals were then interpolated using a linear approach to determine corresponding percentiles for each possible score.
The percentile tables below demonstrate the interpolated values for the Total Internalising and Total Anxiety scores for the different age groups. The descriptors (i.e., Mild, Elevated, and Clinical) are highlighted in colour in the Percentile column.