The K10+ has two subscales, Depression and Anxiety, and can be used as a useful measure to track symptom progression during the course of treatment.
The K10 is also available, which is a 10-item version of the K10+. The K10+ includes additional questions that provide further insights into the individual’s mental health status, covering aspects such as the ability to carry out daily activities and the presence of physical pain, which can also reflect psychological distress levels.
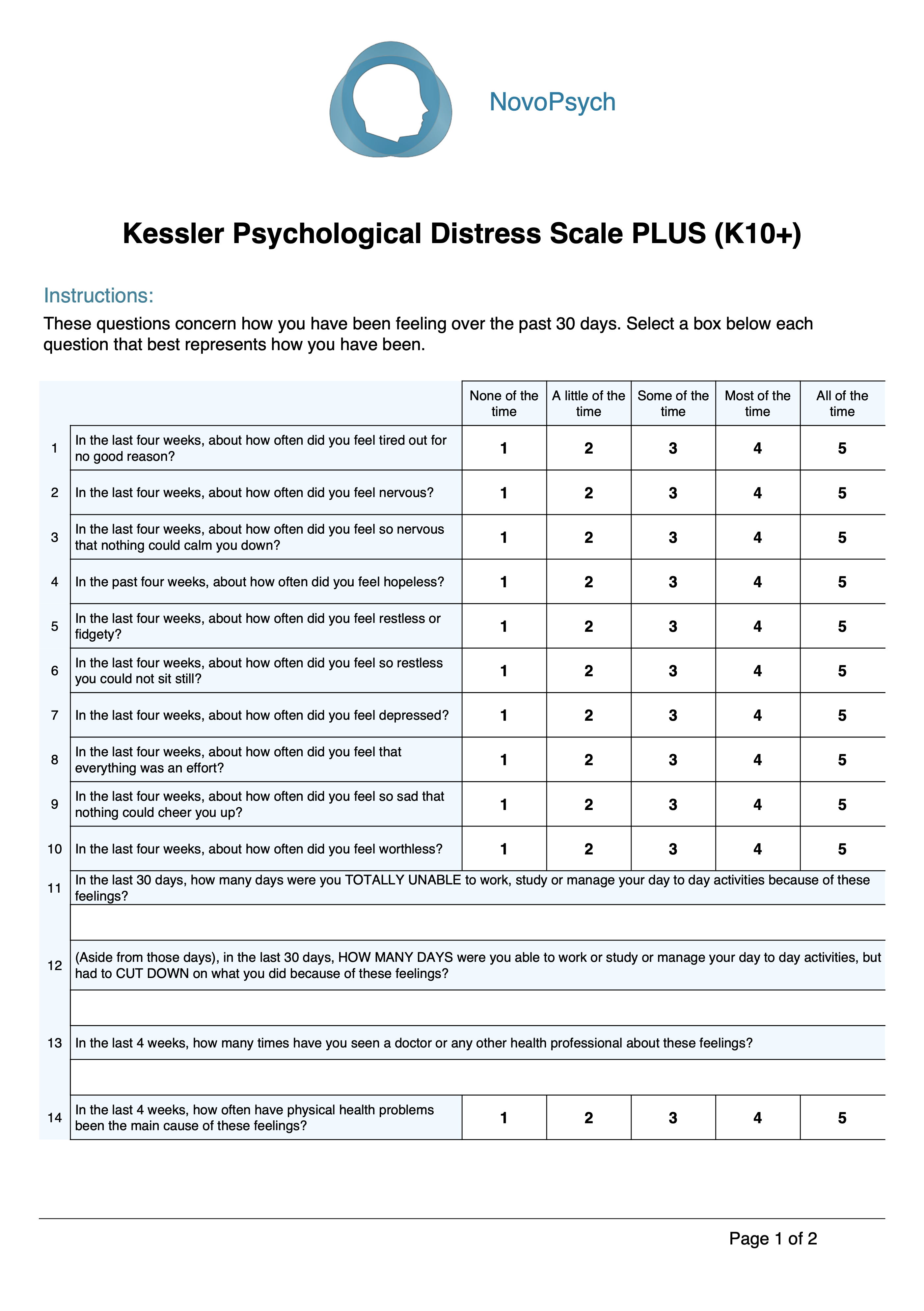
Example K10+ items:
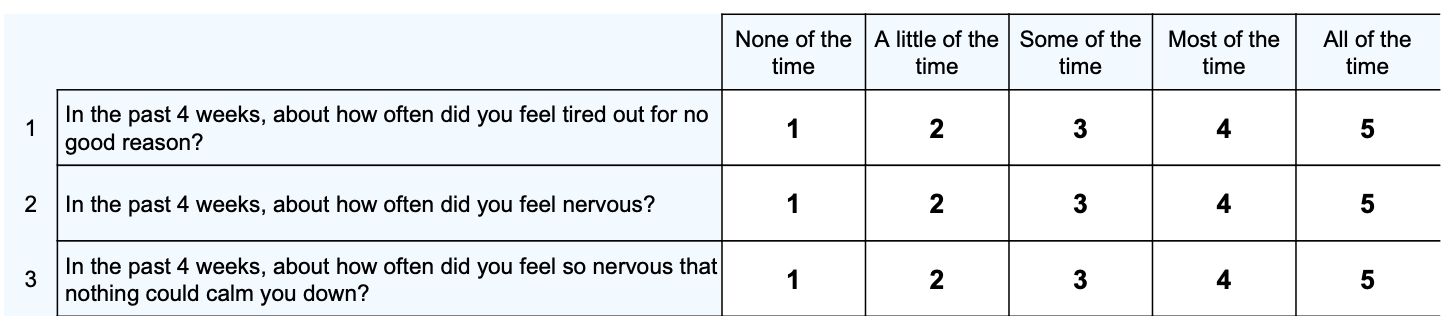
The K10+ is particularly useful for clinicians as it serves both as a screening instrument and a severity measure for mental health issues such as anxiety and depression. The K10+ helps in the rapid identification of individuals who may be suffering from mental health issues, facilitating timely intervention. The scale’s focus on the most recent 30 days ensures that the assessment reflects the current state of the patient’s mental health, which is crucial for effective treatment planning and monitoring of progress over time.
Scores range from 10 to 50 with higher scores indicating a higher severity of psychological distress.
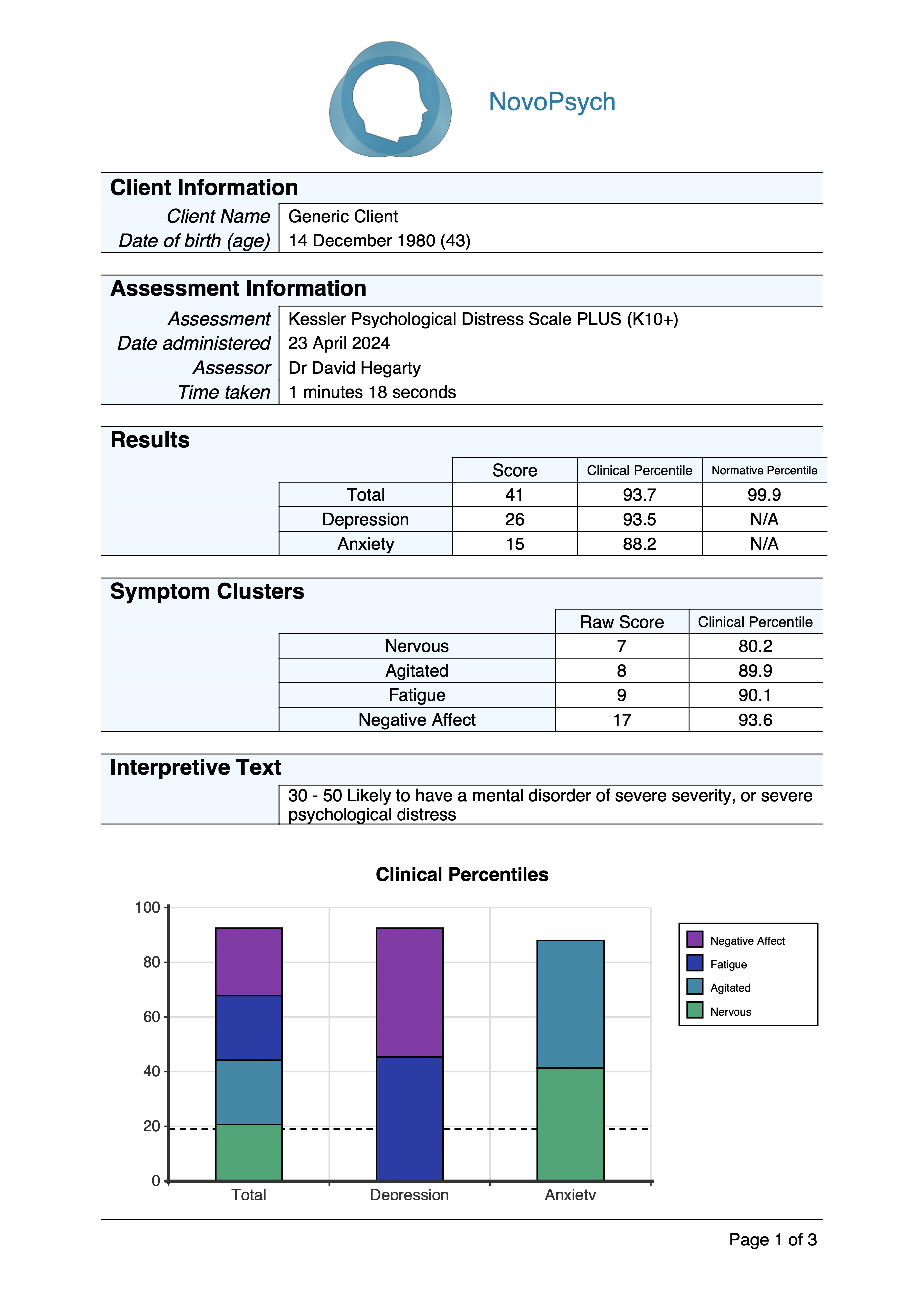
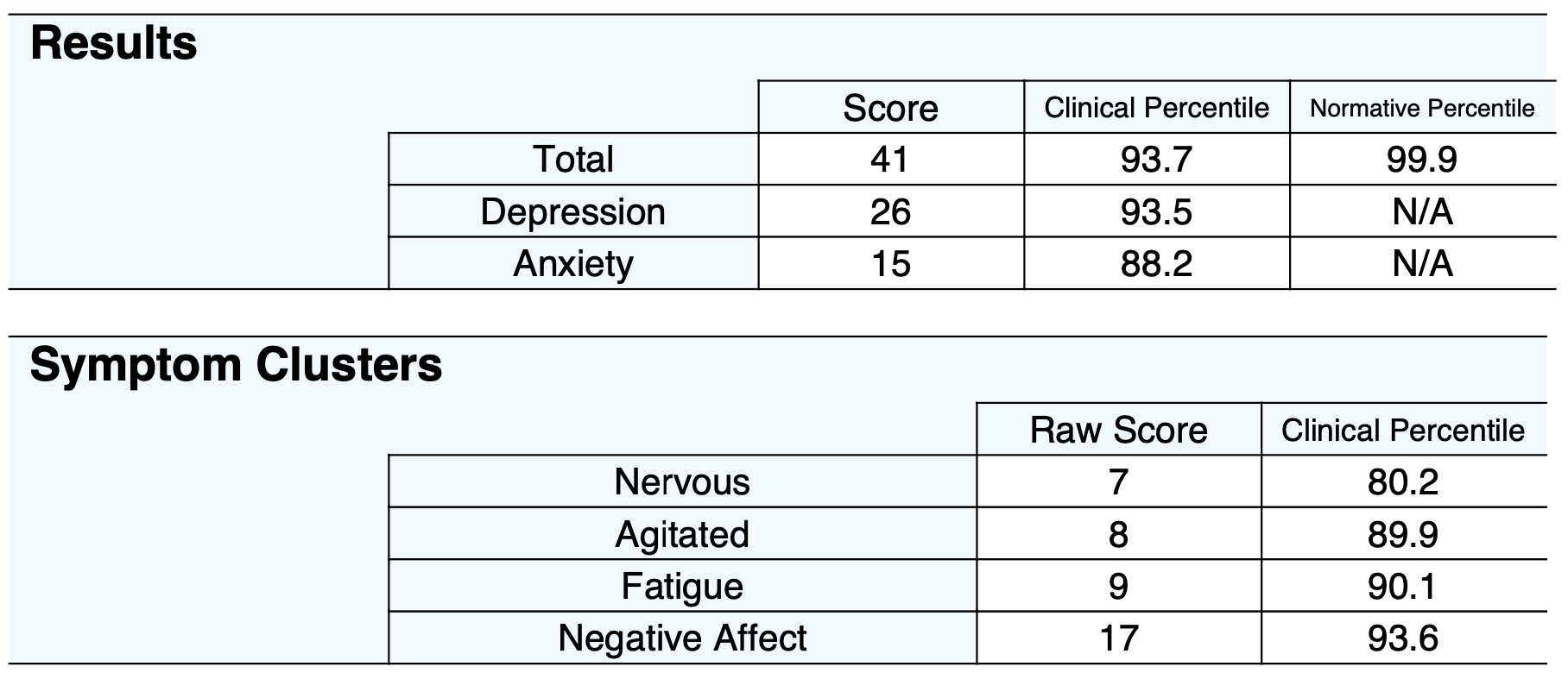
Percentiles are also presented, comparing scores against clinical and normative samples. A Clinical Percentile of around 50 is indicative of typical symptoms for those presenting for psychological treatment, and corresponds to a percentile of 95 on the normative sample.
Total scores can be split into four levels of severity:
The two main subscale scores are also presented:
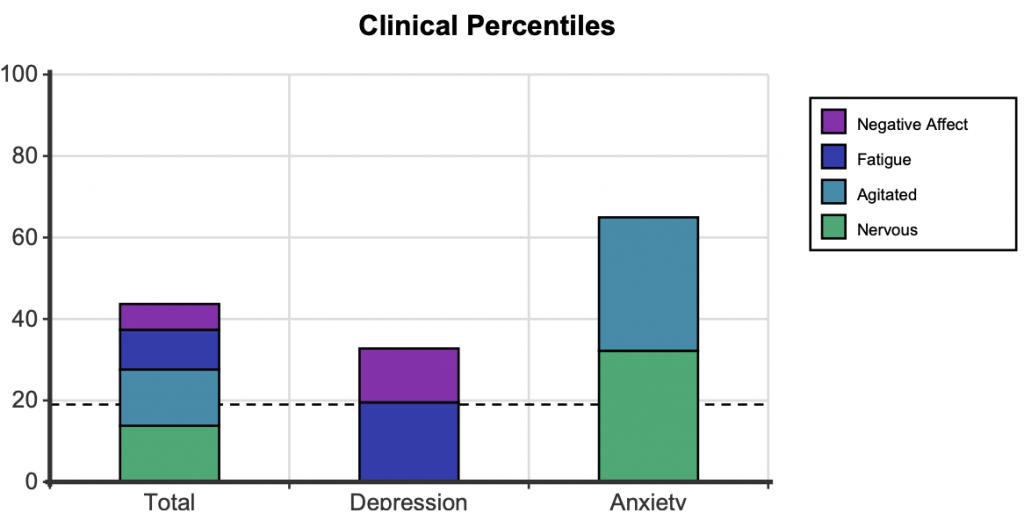
In addition, scores and clinical percentiles are also presented for four first order factors, showing the specific makeup of a patient’s psychological distress.
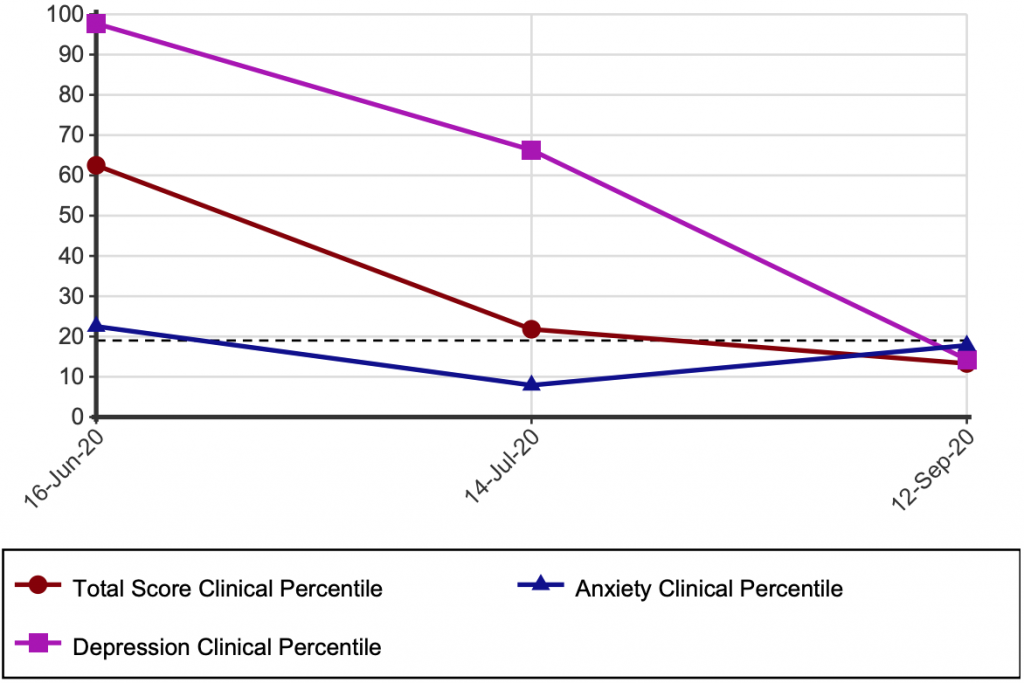
When administered on multiple occasions scores are graphed over time against Clinical Percentiles. The Y axis is from 0 to 100, and represent the percentile rank compared to other individuals seeking psychological intervention. For example, a percentile of 50 would represent the typical score for someone seeing a psychologist. Any scores above the dotted line at the 18.7th percentile indicate scores in the “clinical range”, while those below indicate no or minimal distress.
The K10 has been extensively validated, and scores have strong association between CIDI (WHO Composite International Diagnostic Interview) diagnosis of anxiety and affective disorders. There is a lesser but significant association between the K10 and other mental disorder categories and with the presence of any current mental disorder (Andrews & Slade, 2001).
Sensitivity and specificity data analysis also supports the K10 as an appropriate screening instrument to identify likely cases of anxiety and depression in the community and to monitor treatment outcomes. Normative data in an Australian sample was collected showing a mean score of 14.5 among a non-clinical community population (Slade, Gove & Burgess, 2010).
While the total score of the K10 has been the conventional method for scoring, factor analysis has found four district clusters of symptoms, with two second order factors (Brooks, Beard & Steel, 2006):
Data compiled by NovoPsych (n = 25,171) shows the average score for someone seeking psychological treatment in Australia is 27.1 (SD= 9.1), with a Depression subscale mean of 16.6 (SD = 6.2) and Anxiety mean of 10.5 (SD = 3.8). This data is used to generate Clinical Percentiles.