Dissociation is an adaptive defence in response to high stress or trauma that is characterised by memory loss, depersonalisation, derealisation, identity confusion, and identity alteration. Around 10% of the population will meet criteria for a dissociative disorder during their lifetime (Kate, Hopwood, Jamieson, 2020). Severe forms of dissociation most often begin in childhood and persist or develop further in adolescence (and if not treated, adulthood). The young person may not be aware of the reasons for their difficulties as memories of traumatic and/or overwhelming experiences are often walled off from consciousness.
The MID-60-A has 12 subscales, which are presented here according to the diagnostic category the subscale is most aligned to:
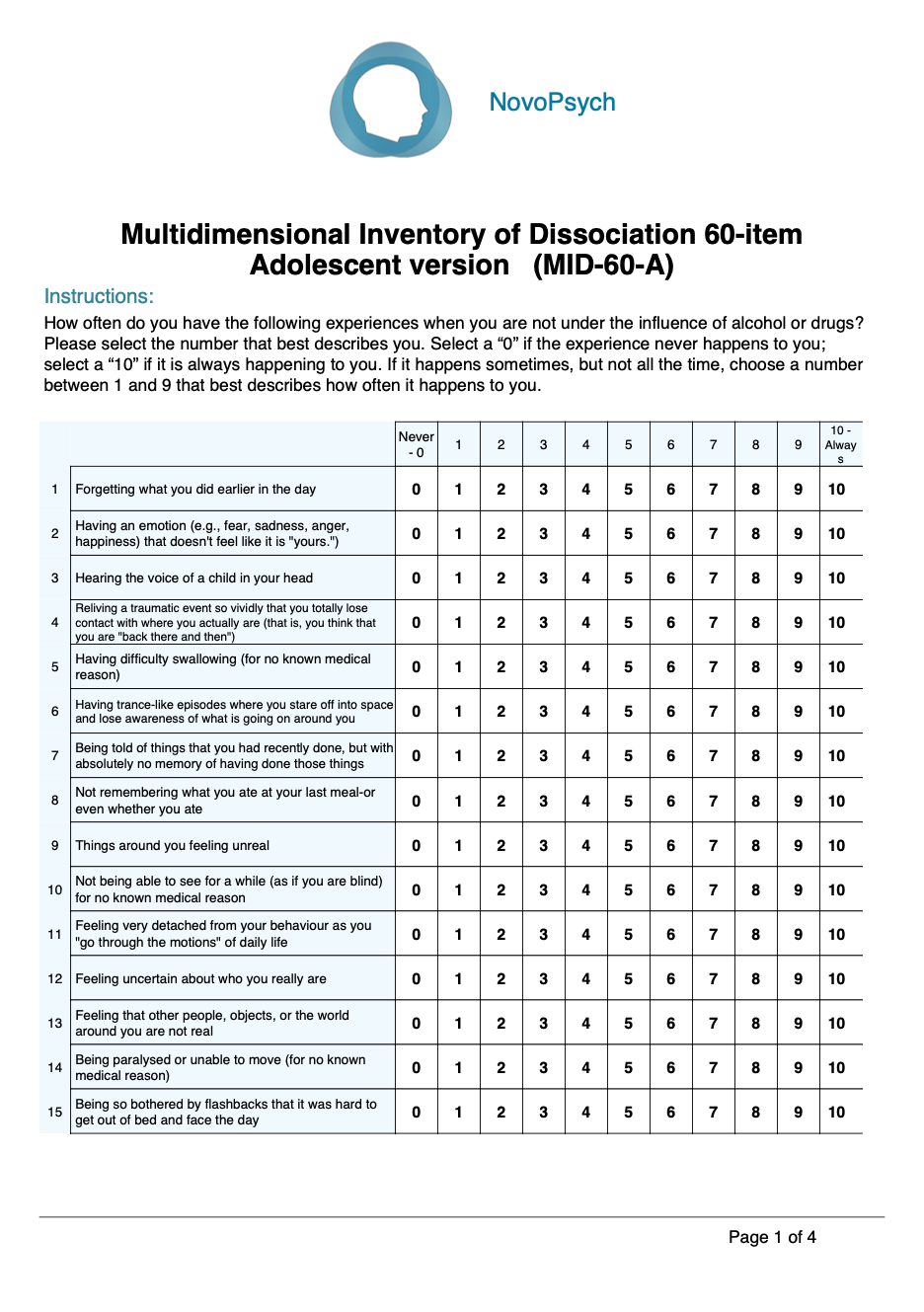
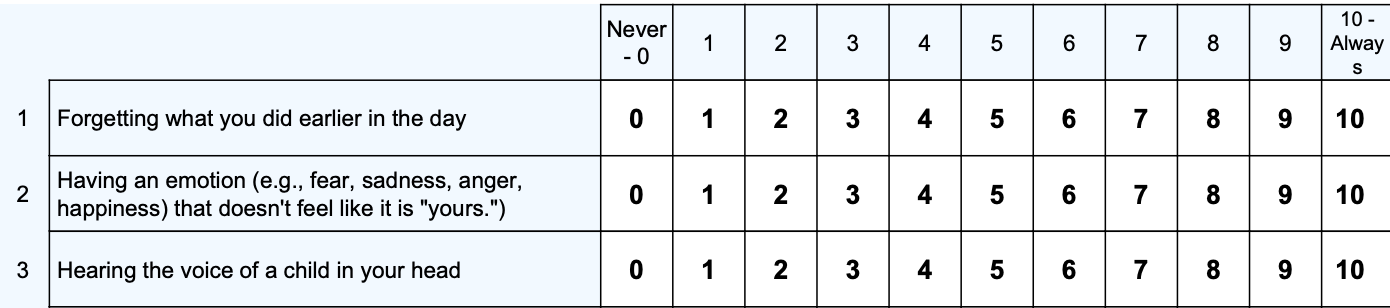
Clients who are completing the MID-60 at home may benefit from further instructions available here.
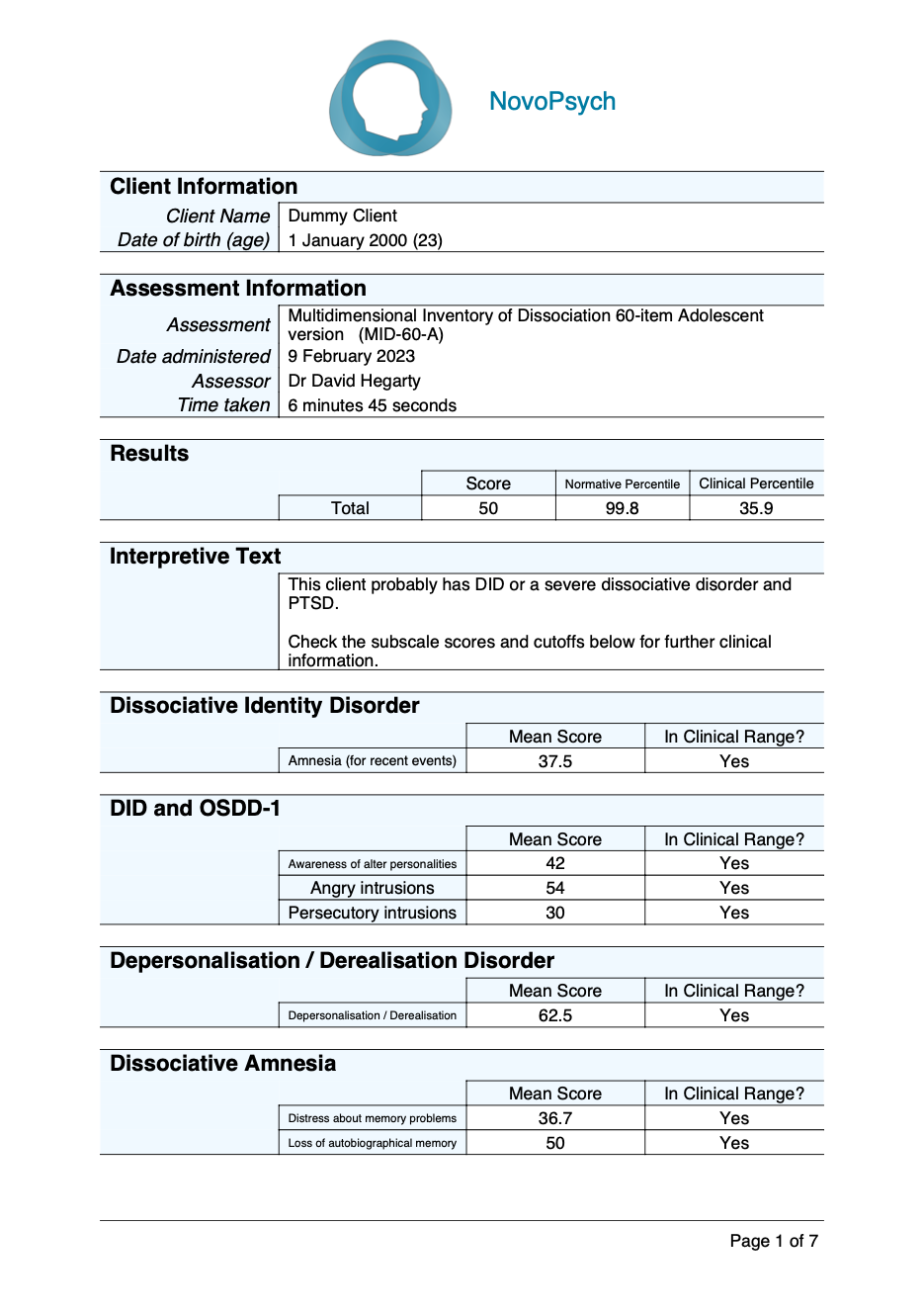
A total mean score (range 0 to 100) is calculated by averaging all 60 responses and multiplying by 10. The mean score represents to total level of dissociative experiences, also interpreted as percentage of time the person self-reports having dissociative symptoms and experiences.
Two percentiles are presented for the total mean score, indicating how the respondent scored in comparison to normative and clinical populations.
The normative percentile provides a comparison against a sample of typical individuals (Kate et al., 2021). A percentile of 50 represents average (and healthy) levels of dissociative experiences. In contrast, a percentile of 90 indicates the respondent scored above 90 percent of typical individuals and is of clinical significance.
The clinical percentile compares the respondent’s score against people who have been diagnosed with a dissociative disorder (Kate, Jamieson & Middleton, 2021; 2022). A clinical percentile of 50 represents pathological levels of dissociation that is typical among those with a dissociative disorder.
Interpretation for the MID-60-A mean scores is as follows:
Subscales
The MID-60-A provides information on subscales relevant to different diagnoses. This enables the clinician to form an impression about the likely diagnosis. For example, a score of 27 is clinically significant, but does not indicate the most likely diagnosis. If the subscales of PTSD and depersonalisation/derealisation are both above the clinical threshold, this can indicate the person has the dissociative subtype of PTSD, whereas if the memory-related subscales are above the clinical threshold this can indicate dissociative amnesia. Another example is a person who has a total mean score of 45, which would seem to indicate dissociative identity disorder. Yet, if the subscale score for amnesia (for recent events) is not elevated, this points towards a more severe case of other specified dissociative disorder.
The subscales are:
The MID-60-A is for screening purposes, is not designed to be the sole determinant of a diagnosis and should always be used in conjunction with clinical expertise. Further evaluations can be conducted with the Structured Clinical Interview for DSM-5 Dissociative Disorders (SCID-D) or Dissociative Disorders Interview Schedule (DDIS).
The MID-60-A is a short version of the 218-item Adolescent Multidimensional Inventory of Dissociation (A-MID; Dell, n.d.) which is a diagnostic instrument based on the adult MID (Dell, 2006). The A-MID uses the same calculations and clinical thresholds as the MID (Dell, Coy, Madere 2006). The MID-60-A was derived from the five items with the highest pattern matrix loading for each of the MID’s 12 factors (Dell & Lawson, 2009). The MID-60 has a nearly identical factor structure to the full MID, excellent internal reliability (α = .97) and content and convergent validity (Kate et al., 2020).
The MID-60-A is identical to the MID-60 aside from minor wording changes to two questions that are not expected to alter overall or subscale scores. The psychometric properties of the MID-60-A are yet to be established.
Normative sample
The MID-60-A scores in a sample of 30 adolescents – university students aged 18 and 19 – found the mean MID-60-A score was 14.0 (SD = 12.7). The scores for this group were not significantly different than participants aged 20 or over (Kate, 2022).
Clinical samples
Females with a dissociative disorder diagnoses (N = 30) had a mean MID-60-A score of 56.8 (SD = 18.8) and the two males had a mean score of 53.4 (SD = 4.7; Kate, Jamieson & Middleton, 2021; 2022). This is consistent with the mean for the 218-item MID, i.e., DID (N = 76, M = 51.3, SD = 18.7) and OSDD-1 (N = 40, M = 39, SD 19.4; Dell et al., 2017). The MID mean has been calculated in people with schizophrenia experiencing a relapse (N = 20, M = 27.0, SD = 20.6) and in remission (N = 20, M = 18.4, SD = 19.2; Laddis & Dell, 2012) and in a clinical group with a borderline personality disorder diagnosis (N = 21, M = 25.4, SD = 18.1, Korzekwa et al., 2009).