Although initially developed for assessing OCD (when hoarding disorder was traditionally encapsulated under the OCD diagnosis), more recent research has established two scales to reliably assess both OCD and hoarding disorder (Wootton et al., 2015). The OCI-R can be used as a screening tool, an aid in diagnosis of both OCD and hoarding disorder, or as a tool to monitor progress in therapy.
The OCI-R has the following subscales:
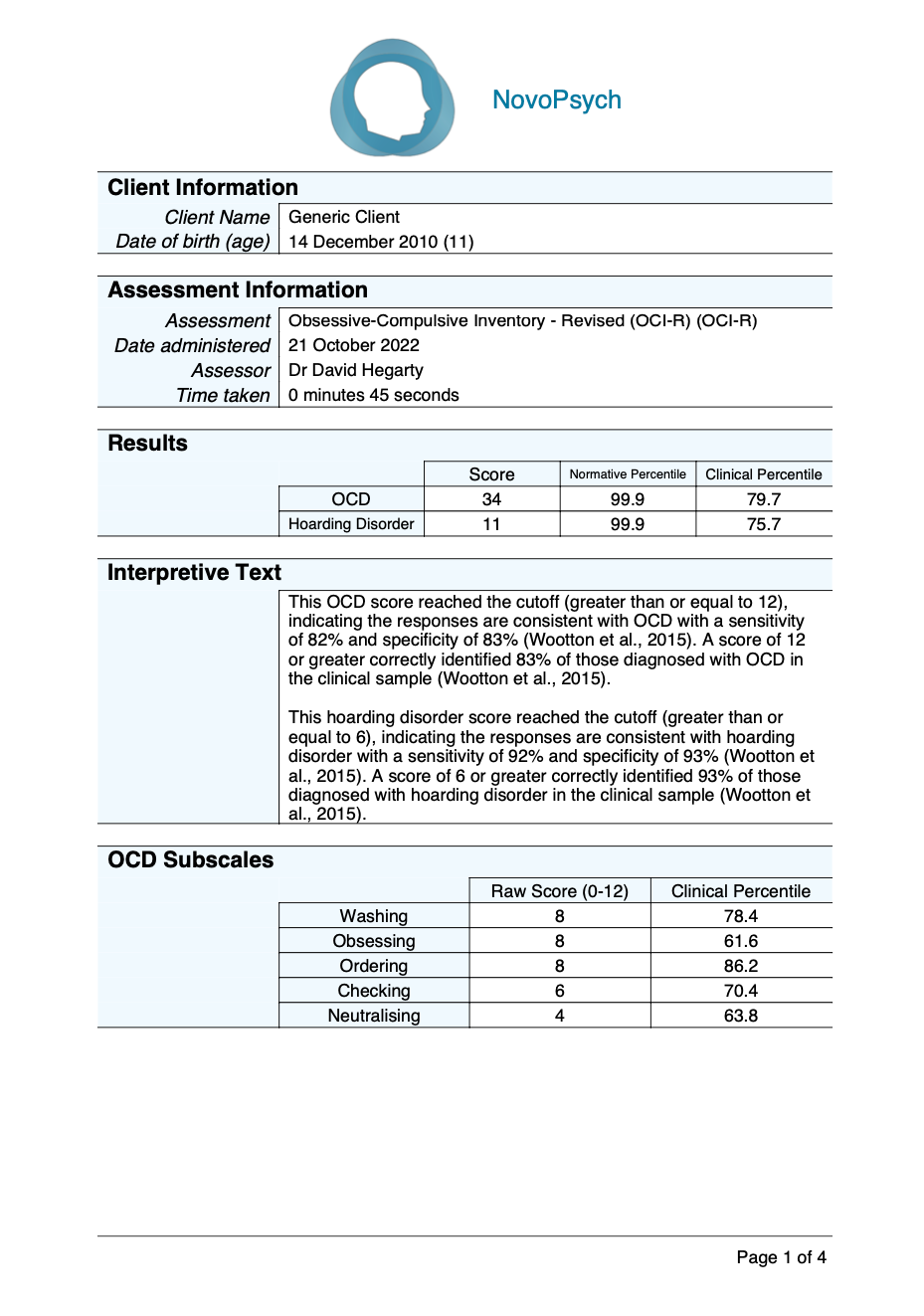
For the OCD component of the OCI-R (items 2, 3, 4, 5, 6, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18), the total score ranges from 0 – 60, with higher scores indicative of more severe OCD symptoms. A cutoff score of 12 is used to determine the likelihood of an OCD diagnosis (with a sensitivity of 82% and specificity of 83%).
Normative and clinical percentiles are presented comparing the respondent’s scores to other adults (Wootton et al., 2015). A normative percentile rank of 50 indicates an average level of OCD symptoms in comparison to the the general population, and is indicative of typical (and healthy) levels of symptomatology. A clinical percentile rank of 50 indicates an average level of OCD symptoms in comparison to the clinical group (with an OCD diagnosis), and is indicative of elevated levels of symptomatology.
For the hoarding disorder subscale of the OCI-R (items 1, 7, 13), the total score ranges from 0 – 12, with higher scores indicative of more severe hoarding symptoms. A cutoff score of 6 is used to determine the likelihood of a hoarding disorder diagnosis (with a sensitivity of 92% and specificity of 93%).
A normative and clinical percentile are presented comparing the respondent’s scores to other adults (Wootton et al., 2015). A normative percentile rank of 50 indicates an average level of hoarding symptoms in comparison to the normative group, and is indicative of typical (and healthy) levels of symptomatology. A clinical percentile rank of 50 indicates an average level of OCD symptoms in comparison to the clinical group (with a hoarding disorder diagnosis), and is indicative of elevated levels of symptomatology.
The OCD component of the OCI-R also reports the client’s score (between 0 – 12) across 6 subscales, with a clinical percentiles comparing the respondent’s scores to a comparison group whom have received a OCD diagnosis (Abramovitch et al., 2020):
The six-factor structure of the OCI-R has been demonstrated consistently across numerous clinical (Gönner et al., 2008; Huppert et al., 2007) and non-clinical samples (Chasson et al., 2013; Solem et al., 2010) and the OCI-R has shown adequate test-retest reliability (Foa et al., 2002; Chasson et al., 2013).
It was found that the OCI-R can be separated into two measures for OCD and hoarding disorder that can differentiate between DSM-5 diagnostic groups (Wootton et al., 2015). The OCD component of the OCI-R correlates more strongly with a measure of anxiety (BAI, r =.61) than with measures of hoarding (SI-R r =.06; HRS r =-.01; Wootton et al., 2015). The hoarding disorder subscale of the OCI-R correlates strongly with the SI-R (r =.94) and HRS (r =.89) and only moderately with a measure of anxiety (BAI, r =.36; Wootton et al., 2015). Cronbach’s alphas for both parts of the OCI-R were high (r = .94 for hoarding disorder and r = .92 for OCD; Wootton et al., 2015).
Receiver operating characteristic (ROC) analyses were conducted in order to ascertain the diagnostic sensitivity (percentage of patients who were accurately identified as having the diagnosis) and specificity (percentage of patients who were accurately identified as not having the diagnosis) of the hoarding disorder and OCD aspects of the ODI-R (Wootton et al., 2015). On the OCD scale a cut score of 12 provided the best balance between sensitivity and specificity, with a false positive rate of 17% and the false negative rate of 18%. The percentage of participants who were correctly classified based on a cut score of 12 was 83%. For the hoarding disorder scale a cutoff score of 6 provided the best balance between sensitivity and specificity. The false positive rate was 7% and the false negative rate was 9%. The percentage of participants who were correctly classified based on a cut score of 6 was 93%.
A sample was used to calculate percentiles for the OCD and hoarding disorder components of the OCI-R. The total sample consisted of 474 adult (age 18 or older) participants (mean age = 47.40; SD = 14.23; 67% female). Of these, 201 had a primary diagnosis of hoarding disorder, 118 had a primary diagnosis of OCD, and 155 were a community sample without a psychiatric diagnosis (Wootton et al., 2015). The means (and SDs) are as follows:
OCD scale (items 2, 3, 4, 5, 6, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18):
Hoarding Disorder subscale (items 1, 7, 13):
To calculate a clinical percentile for OCD subscales, a sample of 1,339 adults with a primary diagnosis of OCD was used (Abramovitch et al., 2020) and the means (and SDs) are as follows: