The SCAS-Parent measures six distinct anxiety dimensions:
For clinicians, the SCAS-Parent offers several distinct advantages. Its comprehensive coverage of anxiety domains makes it particularly valuable for initial assessment and treatment planning. The measure helps clinicians quickly identify specific areas of anxiety that may require intervention, while the subscale structure allows for targeted treatment approaches. The inclusion of multiple anxiety dimensions enables clinicians to track changes in specific symptom clusters over time.
The SCAS-Parent is especially useful in educational and clinical settings where understanding the specific nature of a child’s anxiety is crucial for intervention planning. Its alignment with diagnostic categories helps inform clinical decision-making and can guide referral processes. The scale’s ability to differentiate between various types of anxiety makes it particularly valuable for treatment selection and monitoring intervention effectiveness.
A parallel self-report child version (SCAS-Child) is available, maintaining the same anxiety-focused items. The availability of both child and parent versions enables clinicians to gather multiple perspectives on the child’s anxiety symptoms, enhancing diagnostic accuracy and treatment planning.
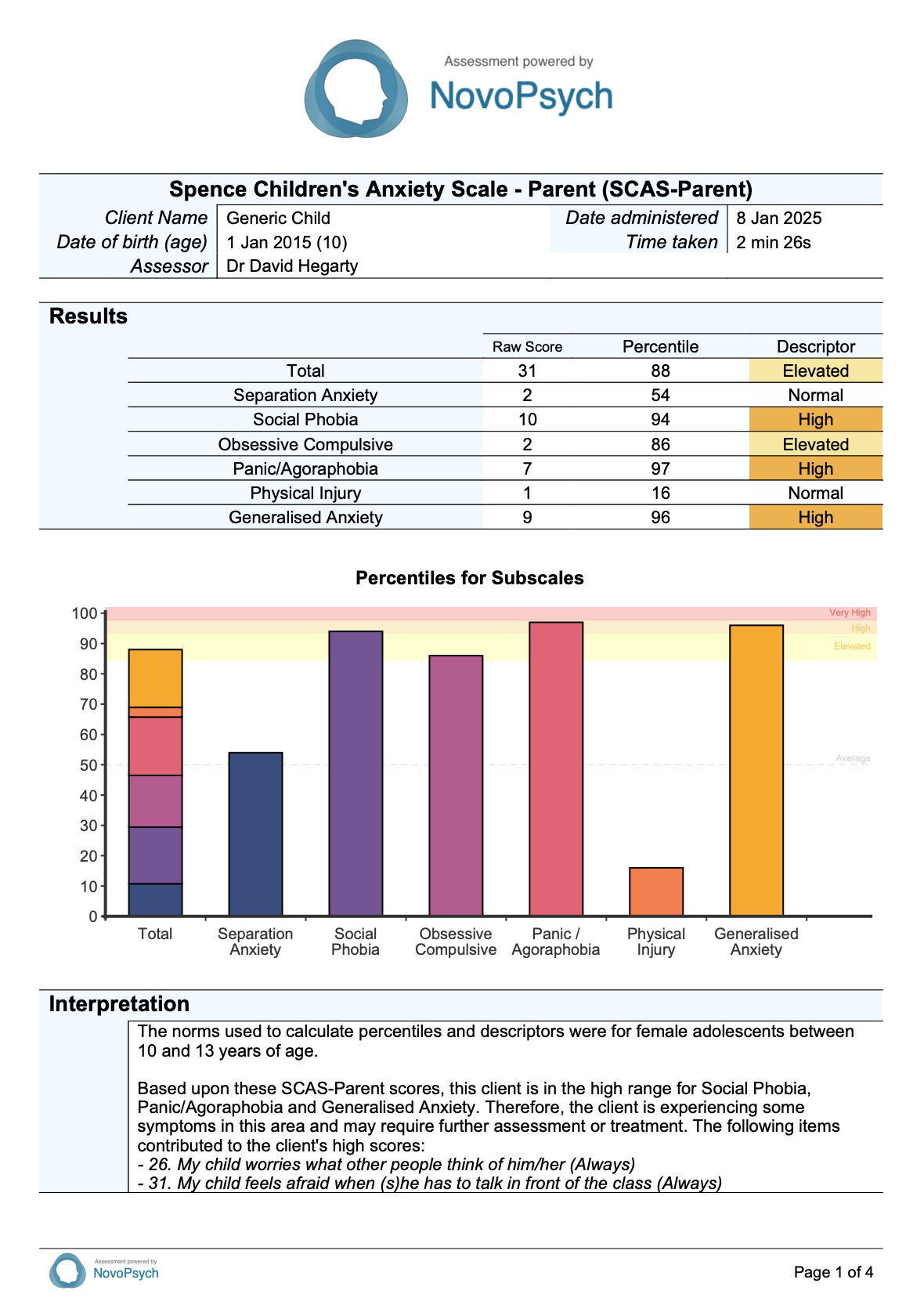
SCAS-Parent scores consist of a total raw score (range from 0 to 114) and six sub-scale scores, with higher scores indicating greater severity of anxiety symptoms. These scores are also converted into percentiles based on age and gender from a large normative sample (N = 1,857) reported by Spence (n.d.) and accessible on www.scaswebsite.com. A percentile score of 85 and above for any subscale score or the total SCAS score indicates elevated and clinically relevant anxiety symptoms.
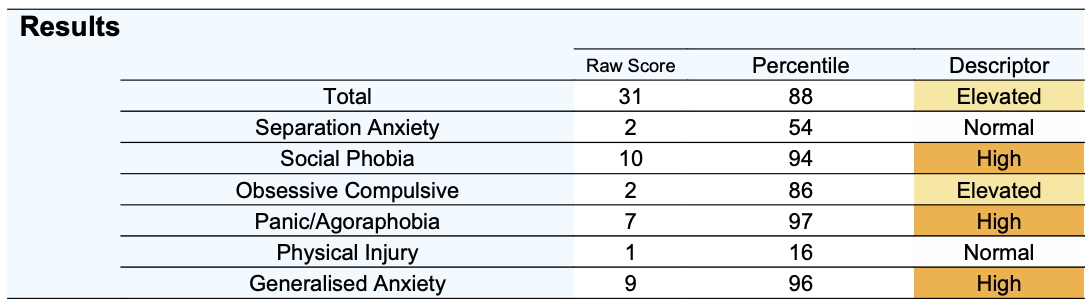
Sub-scales are presented for the SCAS-Parent:
A descriptor is determined that is based upon the percentiles:
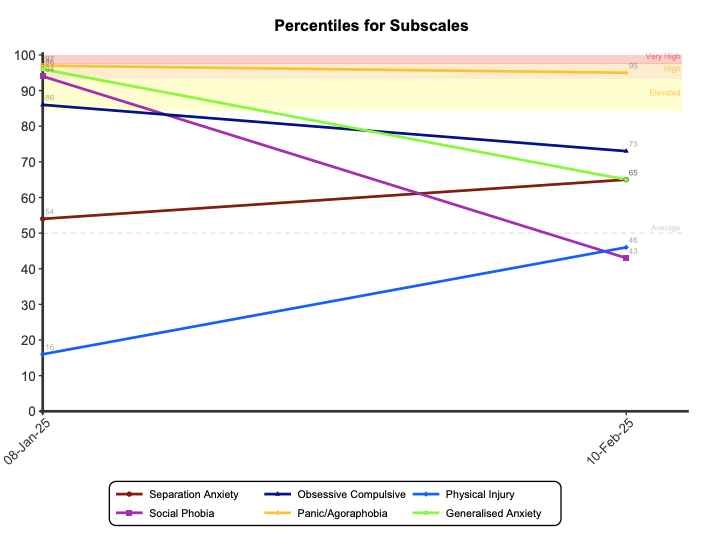
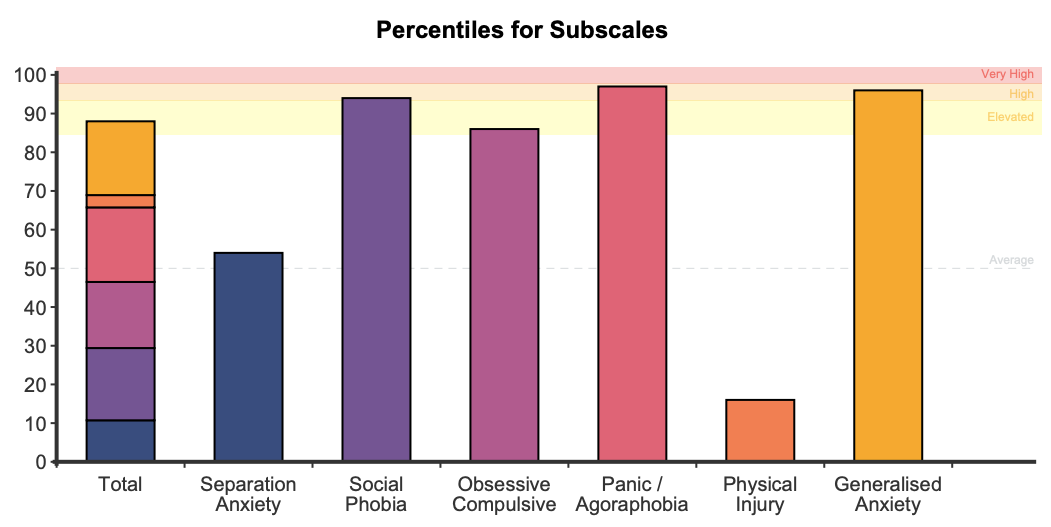
On first administration a stacked bar graph is presented showing the percentiles for the total score and subscales with the descriptors in the background of the plot. If the scale is administered on multiple occasions a graph is produced to track symptoms over time for both the total and the subscale percentiles.
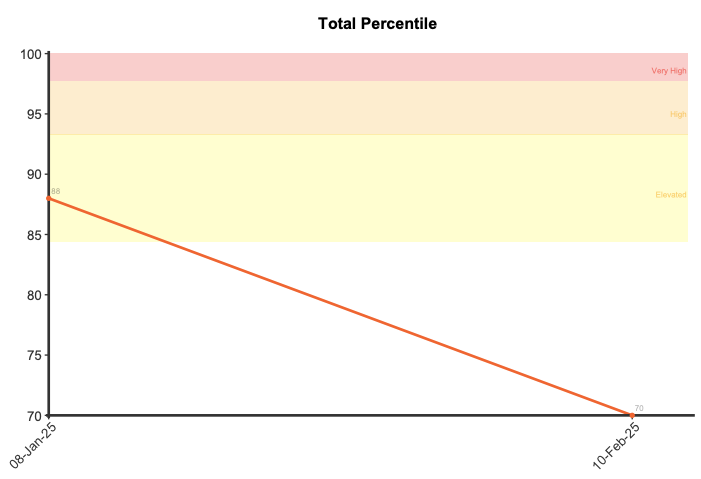
A reliable change score for the total score was determined by NovoPsych based upon 6,099 administrations of the SCAS-Parent. The reliable change score was calculated as 13, meaning that if a client demonstrates a reduction of 13 points or more on the SCAS-Parent total score then they have demonstrated significant improvement in their anxiety symptoms. Similarly, if they have demonstrated an increase of 13 points or more then this indicates a significant deterioration in their anxiety symptoms.
For comprehensive information visit the Spence Children’s Anxiety Scale website at: www.scaswebsite.com
The SCAS-Parent has been extensively validated through numerous studies across multiple countries and cultures. Research has consistently demonstrated robust psychometric properties across clinical and community samples, with particularly strong evidence for its reliability and validity.
Confirmatory factor analyses support a six-factor structure for the SCAS-Parent that corresponds with DSM anxiety disorders: separation anxiety, social phobia, generalised anxiety, panic/agoraphobia, obsessive-compulsive disorder, and physical injury fears (Nauta et al., 2004). The SCAS-P demonstrates excellent internal consistency for the total scale (α = .87-.90) across clinical and community samples (Brown-Jacobsen et al., 2011; Whiteside et al., 2012). Subscale reliability coefficients range from α = .60-.87, with the Physical Injury subscale showing consistently lower reliability across studies.
The SCAS-Parent shows good convergent validity with other measures of child anxiety, including moderate to strong correlations with the Child Behavior Checklist-Internalising scale (r = .55-.59) and discriminant validity is supported by lower correlations with externalising problems (r = .33-.34; Nauta et al., 2004). The OCD subscale correlates significantly with the Children’s Yale-Brown Obsessive Compulsive Scale (r = .36-.44) and OCD symptom ratings from structured diagnostic interviews (r = .58-.67; Whiteside et al., 2012). The parent-report version demonstrates particularly strong validity for identifying OCD symptoms, with 95% sensitivity and 54% specificity in clinical samples.
Parent-child agreement on the SCAS (using both the Parent and Child versions) is moderate to high for most anxiety disorder symptoms. Correlations between parent and child reports range from r = .60-.74 for corresponding subscales, with particularly strong agreement on the OCD (r = .60) and separation anxiety (r = .74) subscales (Brown-Jacobsen et al., 2011). Agreement tends to be higher for observable symptoms (e.g., separation anxiety) compared to internal experiences (e.g., generalised anxiety; Magiati et al., 2017).
The SCAS-Parent effectively discriminates between children with anxiety disorders and non-anxious controls, with correct classification rates of 80-86% (Nauta et al., 2004). The measure also shows reasonable ability to differentiate between specific anxiety disorders, particularly for separation anxiety (70%), social phobia (60%), panic/agoraphobia (68%), and OCD (72%), though it has more difficulty discriminating generalised anxiety disorder (31%; Nauta et al., 2004). In clinical settings, the SCAS-Parent demonstrates good positive predictive value (PPV = .43) and excellent negative predictive value (NPV = .85) across subscales. The OCD subscale shows particularly strong diagnostic utility, with parent reports correctly classifying 72% of cases and demonstrating significant sensitivity to treatment effects (Whiteside et al., 2012).
The SCAS-Parent has been validated in a large sample of children (N = 1,857) in the USA, Australia, and the UK (Brown-Jacobson et al., 2011; Cresswell et al. (n.d.); Nauta et al., 2004; Whiteside et al., 2012). This data is used to determine percentiles that are based upon age (7 – 9, 10 – 13 years of age, or combined (i.e., 7- 13) if the client’s age is outside of these ranges) and gender (male, female, or combined if gender is not specified).
A descriptor is determined that is based upon the percentiles:
A reliable change score has been determined by NovoPsych for the SCAS-Parent total score from data collected between July 2014 and January 2025 where clients had completed multiple assessments. All data was included in the analysis, so no data was removed based upon initial symptom severity. The resultant sample size was 6,099. The reliable change score was calculated using the Jacobson-Truax method of clinical significance classification (Jacobson & Truax, 1991) using a calculated Cronbach alpha from the NovoPsych data. The internal reliability calculated for the Total Score was 0.92 and the reliable change score calculated was 13.