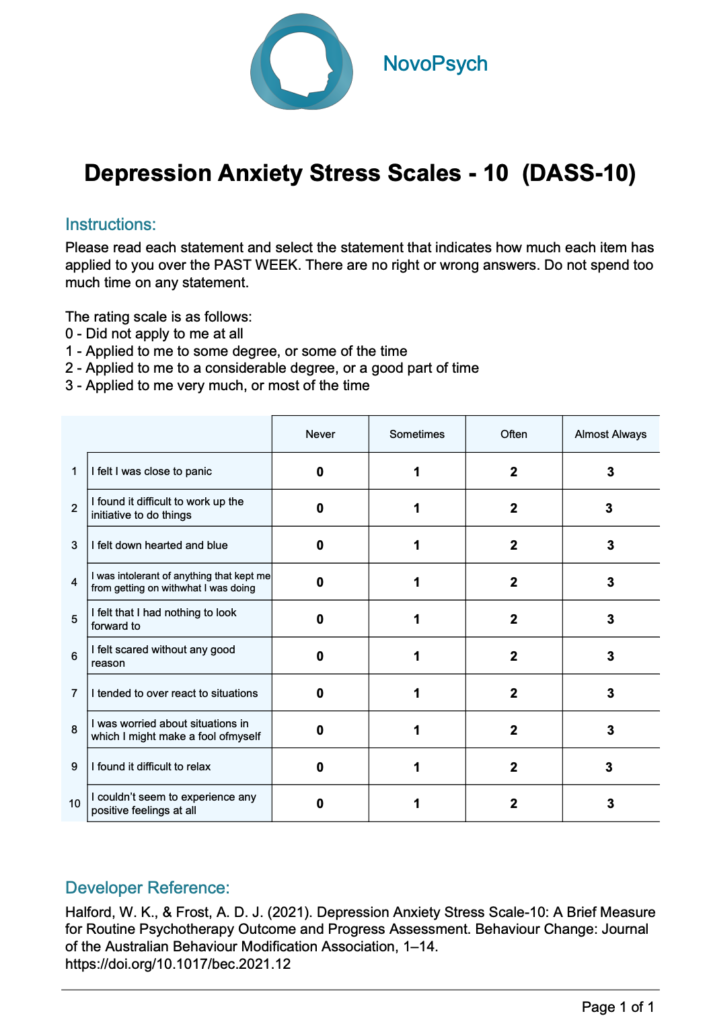
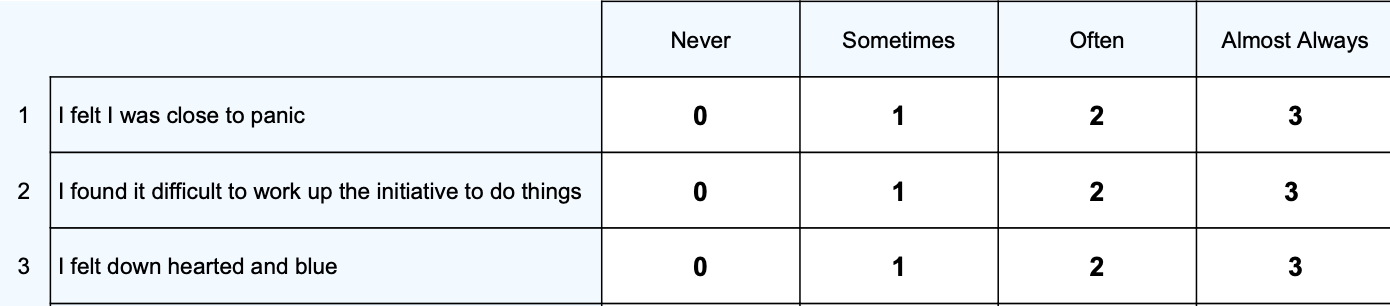
The scale has 10 items taken from the DASS-42, with the addition of two extra items screening for substance use and suicidal ideation. Items 11 and 12 don’t contribute to the overall score but are useful in identifying risks.
The scale was designed to be used for routine outcome monitoring in psychology practices and other mental health settings. It provides an overall level of distress that is sensitive to clinical change and can be used to track the effectiveness of treatment.
Example DASS-10 Items:
The total score for questions 1-10 represents overall distress (0 to 30), with higher scores indicating more severe or greater number of symptoms. Two subscales are presented:

In addition to the raw score being computed, average scores are calculated by dividing the raw score by the number of items, giving a sense of the general pattern of responding at the subscale level. Average scores are helpful for interpretation as they allow comparisons between total score and subscales.
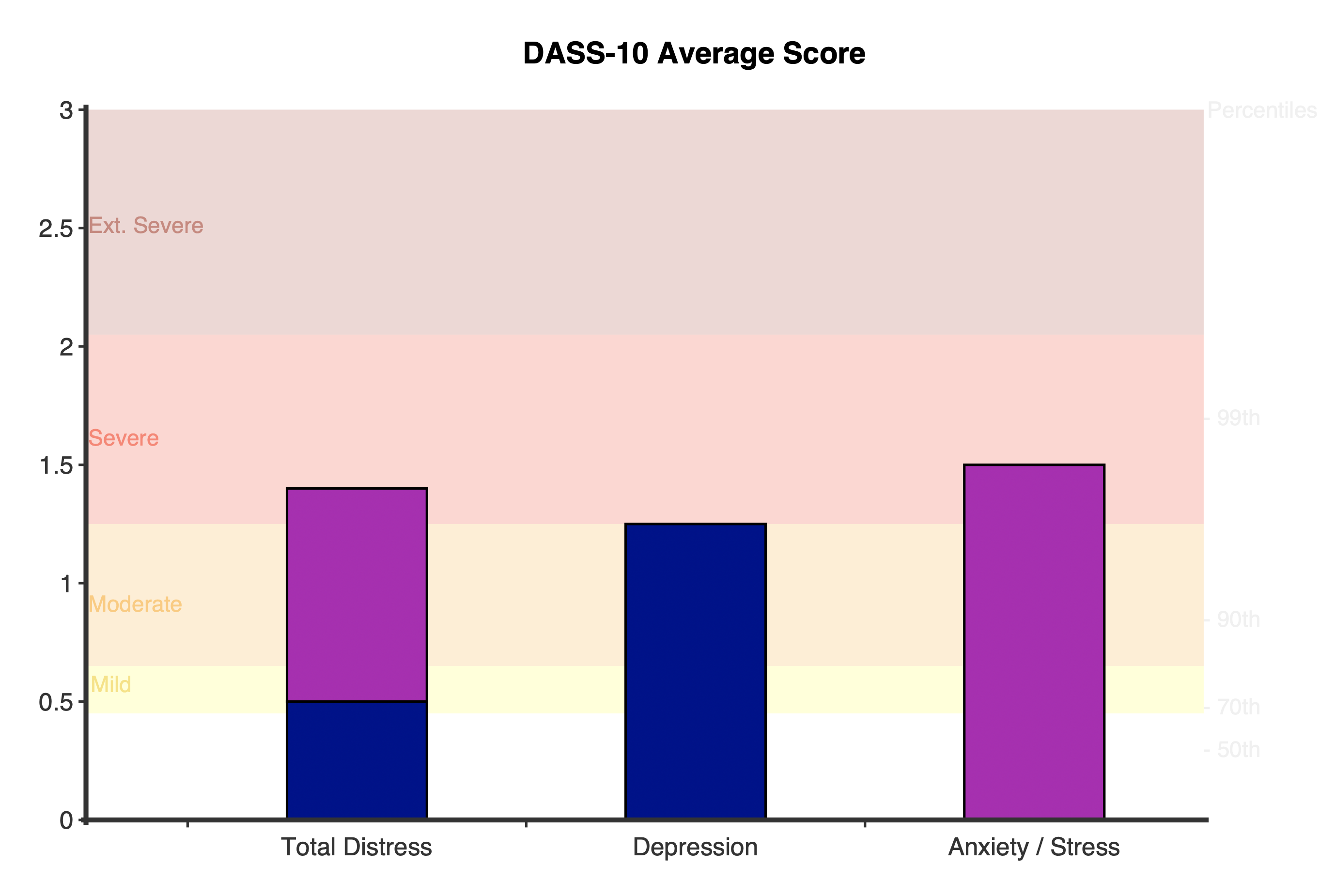
Overall scores can be classified into three severity groups:
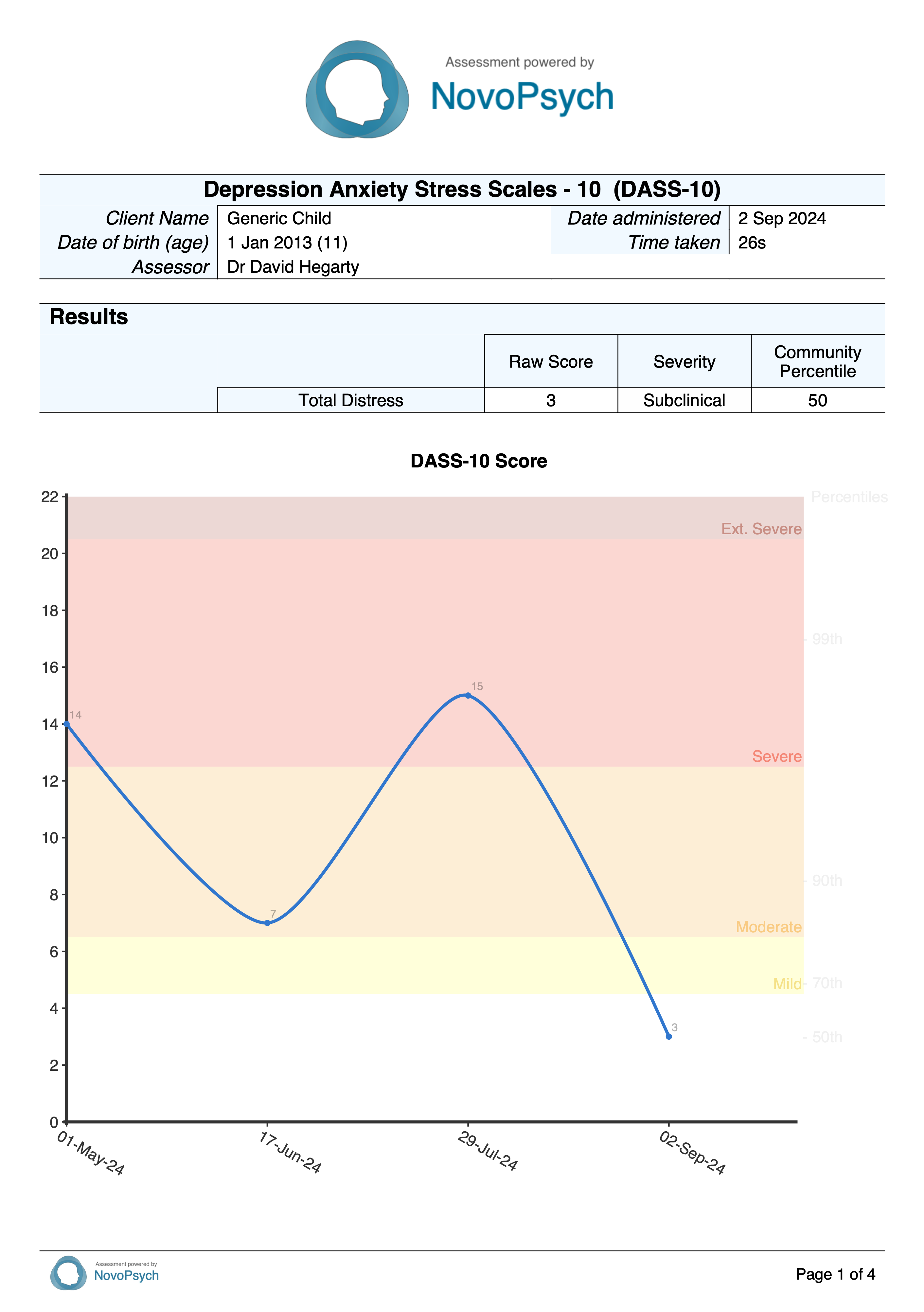
A normative percentile is computed based on a community sample (Halford & Frost, 2021), indicating how the respondent scored in relation to a typical pattern of responding for adults. For example, a percentile of 83 or less indicates the individual has more distress than 83 percent of the normal population, but this puts them in the mild category. In mental health settings it is typical to see people with percentiles in the 90s.
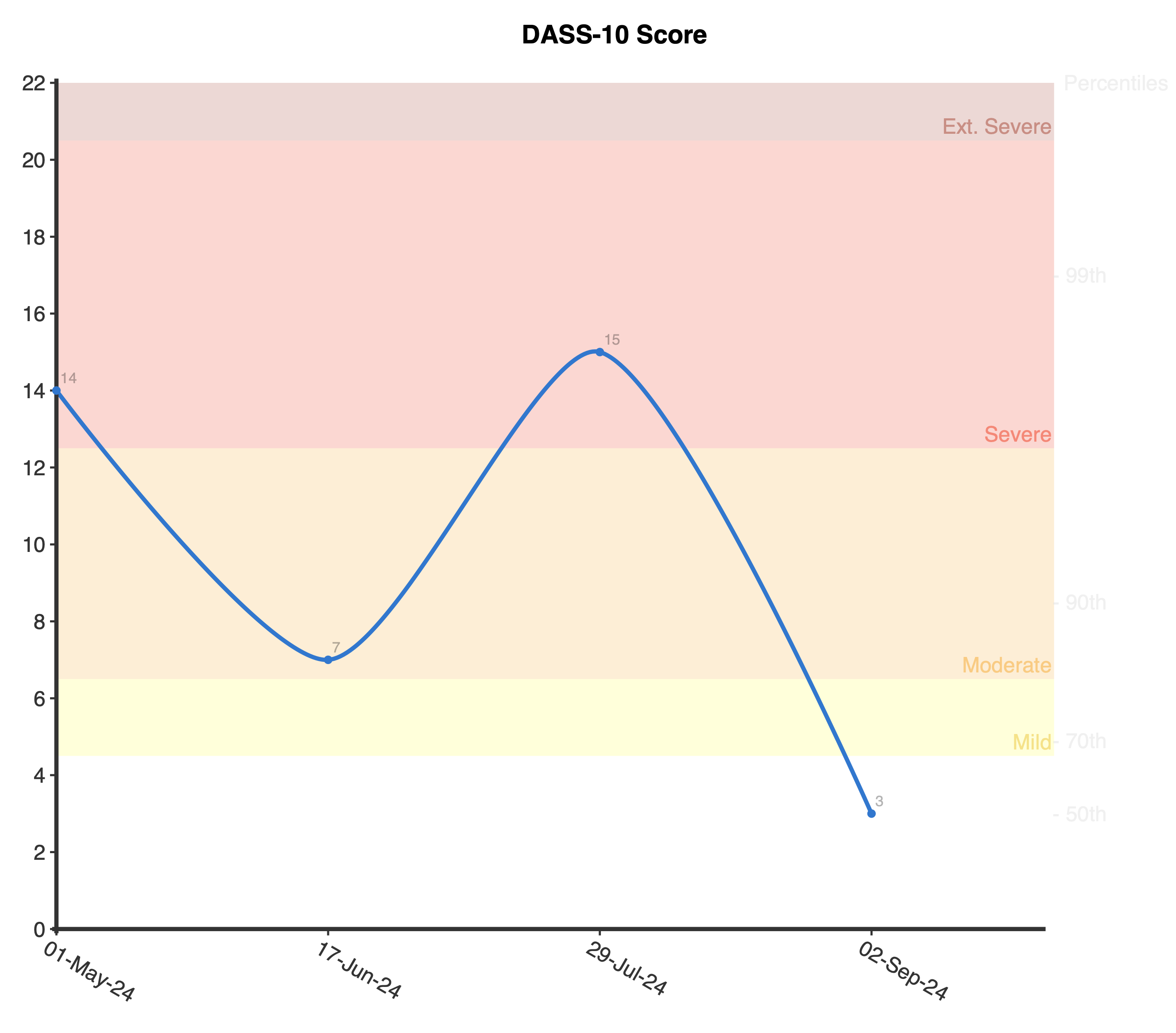
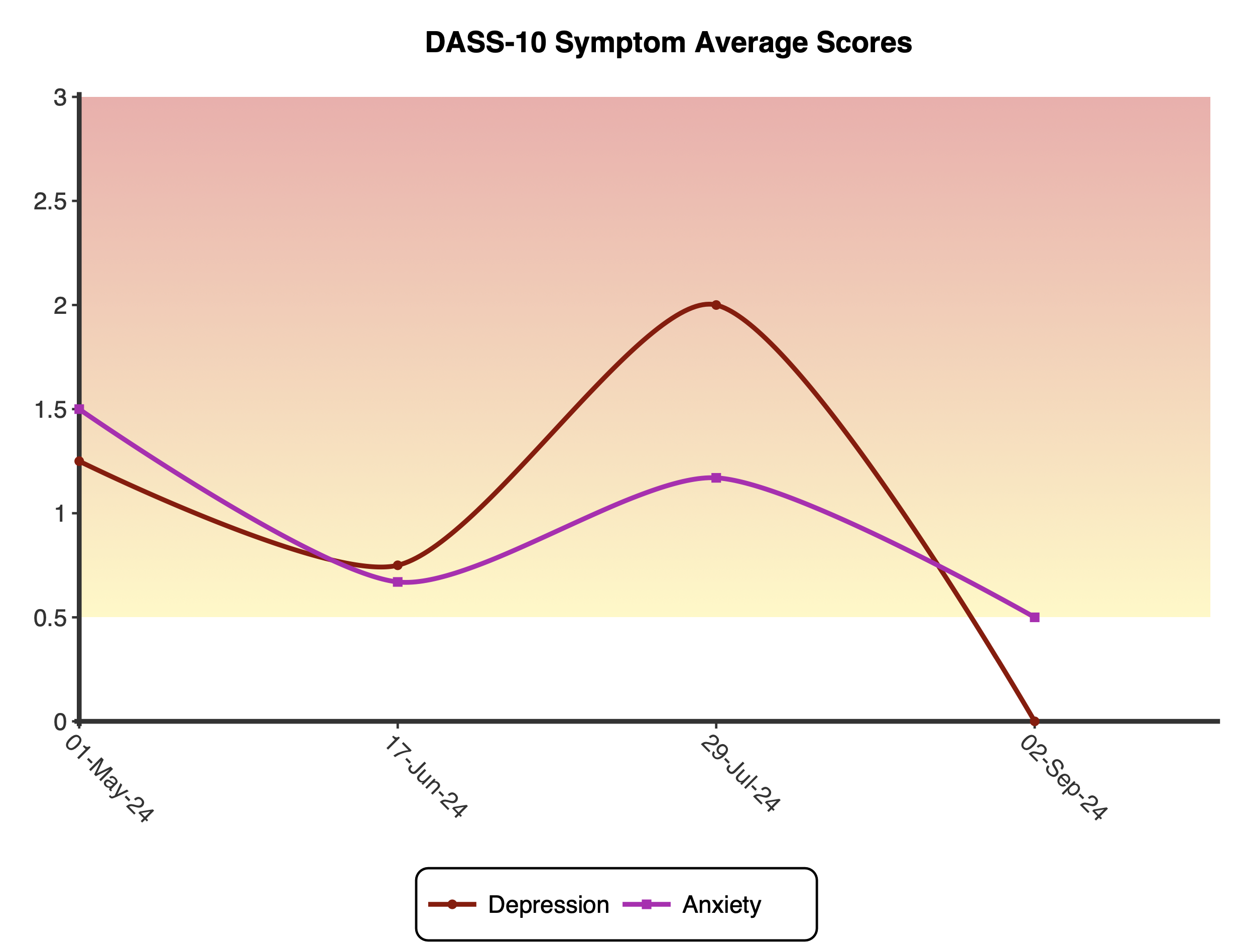
When administered more than once, average scores are graphed, showing the change in symptoms over time.
Based on reliable change calculations, interpretive text is provided describing the respondent’s change in symptoms from first to last administrations, as either having experienced:
The last two questions are used by clinicians to determine whether the client has a potential substance use issue (Question 11) or whether the client has had suicidal ideation (Question 12). Both these items do not contribute towards the overall score or subscale scores, but are highlighted in the the Interpretive Text section if any problems are reported.
Halford and Frost (2021) developed the DASS-10 as a shorter version of the original DASS-42 (Lovibond & Lovibond, 1995). EFA and CFA yielded two highly correlated factors: Anxiety-Stress and Depression subscales. Both subscales and the higher-order Distress factor had high internal consistency (Cronbach’s alpha = 0.83, 0.85, & 0.89 respectively; Halford & Frost, 2021).
Based on the above psychometric properties, reliable change was determined to be a five or more point change between first and last DASS-10 administration.
As expected, the validation study found the DASS-10 was able to discriminate between populations, with a clinical sample scoring significantly higher (mean = 7.67, SD = 4.36) than a community sample (mean = 3.01, SD 3.15). The community sample of newly wedded couples (n = 376) can be used to compute normative percentiles, although because this sample had a significant positive skew, NovoPsych could not use the mean and standard deviation to calculate percentiles. Instead, NovoPsych adjusted the percentiles to match a negative binomial distribution (similar to the ‘contagious Poisson’ distribution) as might be expected for this kind of data (Swanson et al., 2012). Prior to selecting the negative binomial distribution, a comparison between linear, normal, gamma, log-normal and negative binomial distributions was made using models constructed with the known statistics for this sample. As a result of this comparison, the negative binomial distribution best fitted the data due to the skew, over-dispersion, and fit, and it was these modelled percentiles that are used.
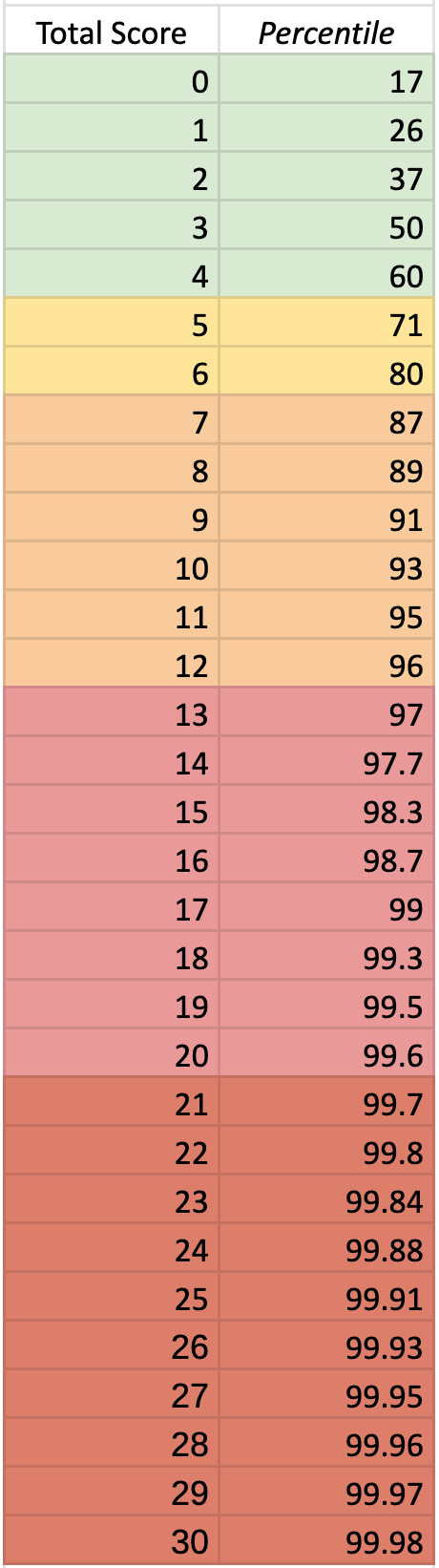
The table below illustrates the calculated percentiles for the total score on the DASS-10. NovoPsych modelled these percentiles using a negative binomial distribution using known corresponding score-percentile combinations. The mean and standard deviation couldn’t be used to calculated percentiles given the significant positive skew of the data. The colours in the background of the percentiles match the descriptors (subclinical = green; mild = yellow; moderate = orange; severe = pink; extremely severe = red).