Worries about health are a normal human experience, and thought to fall along a continuum in the general population (Salkovskis and Warwick, 2001). Towards the upper end of the continuum, individuals are likely to experience and obsessional fear of illness and may fall in the realm of health anxiety. Health Anxiety (now referred to as Illness Anxiety Disorder in the DSM-5-TR and previously known as hypochondriasis) refers to inappropriate or excessive fears about one’s health. It is characterised by excessive fears or beliefs that one has a serious illness, and this is often based on the misinterpretation of bodily sensations or symptoms.
Health anxiety consists of distressing emotions (such as fear) due to thoughts of danger and physiological arousal (Taylor, & Asmundson, 2004). This anxiety is often maintained by behaviours that individuals use to decrease distress however inadvertently increase or maintain physical symptoms of anxiety (Haig-Ferguson et al., 2021). Health anxiety has also been conceptualised to offer a unifying perspective on the fears symptoms worsening or returning commonly experienced by those living with chronic disease (Lebel et al., 2020; Haig-Ferguson et al., 2021).
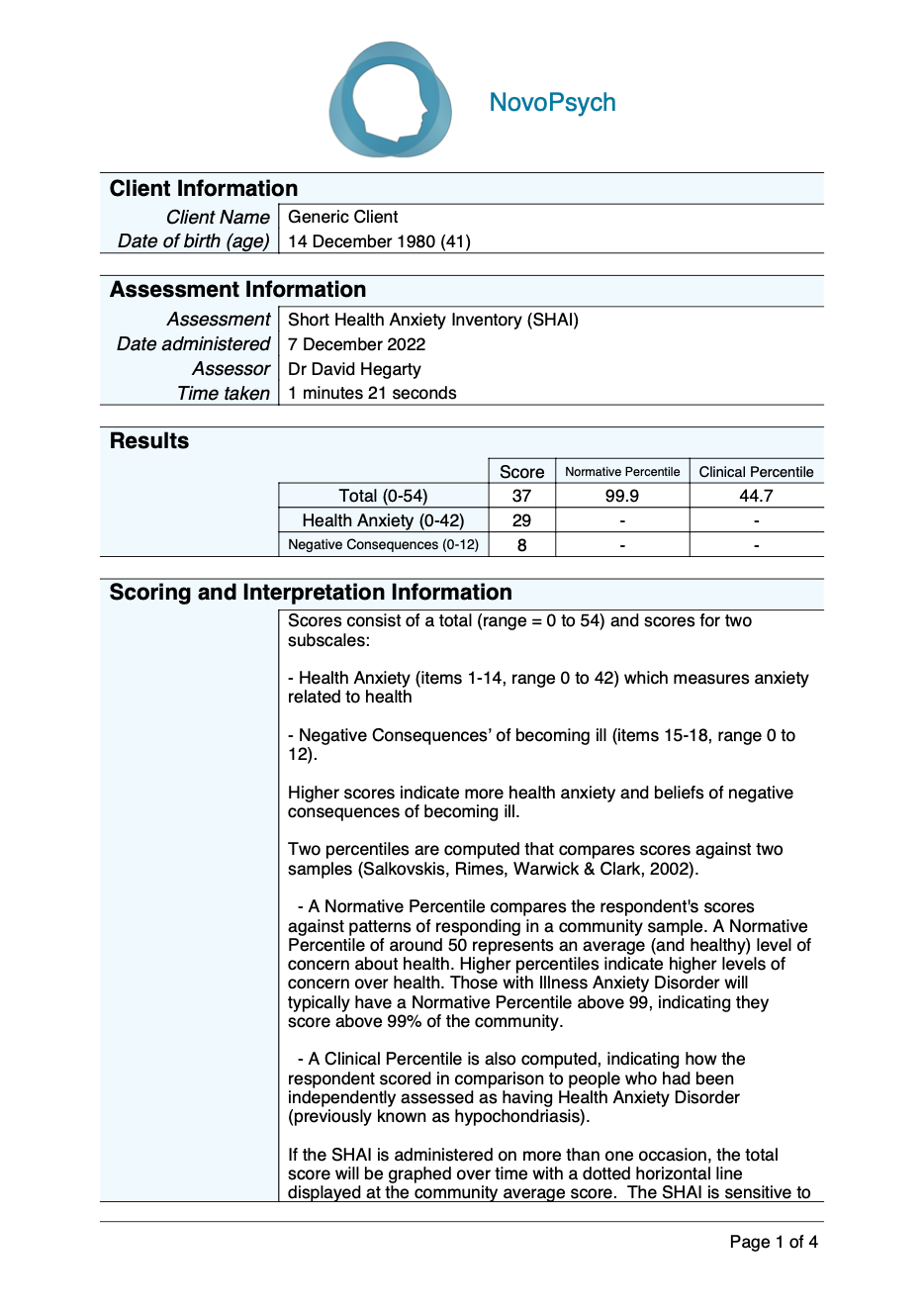
Scores consist of a total (range = 0 to 54) and scores for two subscales:
– Health Anxiety (items 1-14, range 0 to 42) which measures anxiety related to health
– Negative Consequences’ of becoming ill (items 15-18, range 0 to 12).
Higher scores indicate more health anxiety and beliefs of negative consequences of becoming ill.
Two percentiles are computed that compares scores against two samples (Salkovskis, Rimes, Warwick & Clark, 2002).
– A Normative Percentile compares the respondent’s scores against patterns of responding in a community sample. A Normative Percentile of around 50 represents an average (and healthy) level of concern about health. Higher percentiles indicate higher levels of concern over health. Those with Illness Anxiety Disorder will typically have a Normative Percentile above 99, indicating they score above 99% of the community.
– A Clinical Percentile is also computed, indicating how the respondent scored in comparison to people who had been independently assessed as having Health Anxiety Disorder (previously known as hypochondriasis).
If the SHAI is administered on more than one occasion, the total score will be graphed over time with a dotted horizontal line displayed at the community average score. The SHAI is sensitive to treatment effects, it is also a useful measure of the effectiveness of treatment for health anxiety.
Salkovskis, Rimes, Warwick, and Clark (2002) developed the Health Anxiety Inventory (HAI; 64 items) and a shortened version of this scale, the Short Health Anxiety Inventory (SHAI; 18 items), to be sensitive to both normal levels of health concern and severe health anxiety.
The scale was validated in clinical and non-clinical samples, 24 diagnosed with hypochondriasis, 19 anxious controls (panic disorder or social anxiety), 107 women attending a general practice clinic, 267 people attending gastroenterology department, 97 attending MRI scan, 190 non-anxious controls and 66 students. These samples yielded the following means and standard deviates.
– Hypochondriasis patients – 37.9 (SD=6.8)
– Anxious control -18.5 (SD=7.3)
– Controls 12.2 (SD=6.2)
– Students 12.6 (SD=5.0)
– Women in GP clinic 14.5 (SD=5.9)
– Gastroenterology clinic 13.9 (SD=7.4)
Another study found the mean score for SHAI in non-clinical sample with 467 undergraduate students was 10.79 (SD = 6.38) (Abramowitz et al., 2007).
A systematic review and meta-analysis of the SHAI concluded that it was a psychometrically sound tool for assessing health anxiety across non-clinical, clinical, and medical samples (Alberts et al., 2013).
The SHAI has good to excellent internal consistency (= .74–.96) across 16 studies (Alberts et al., 2013). It has sound factorial,, convergent, divergent and criterion validity (Alberts et al., 2013). However, test re-test reliability of the SHAI was reported in only one study by Olatunji et al. (2011) and was found to be adequate (r = .87) when administered over four administrations across a 3-week study period.
The SHAI has also been shown to be sensitive to treatment effects with CBT for severe health anxiety (Williams et al., 2011; Hedman et al., 2011).