A notable strength of the SRS-3-B lies in the fact that it was derived from qualitative research on clients’ reactions to significant events in psychotherapy sessions (Řiháček et al., 2023). Therefore, it contains categories that clients themselves are likely to consider important and, thus, can easily rate from their own perspective.
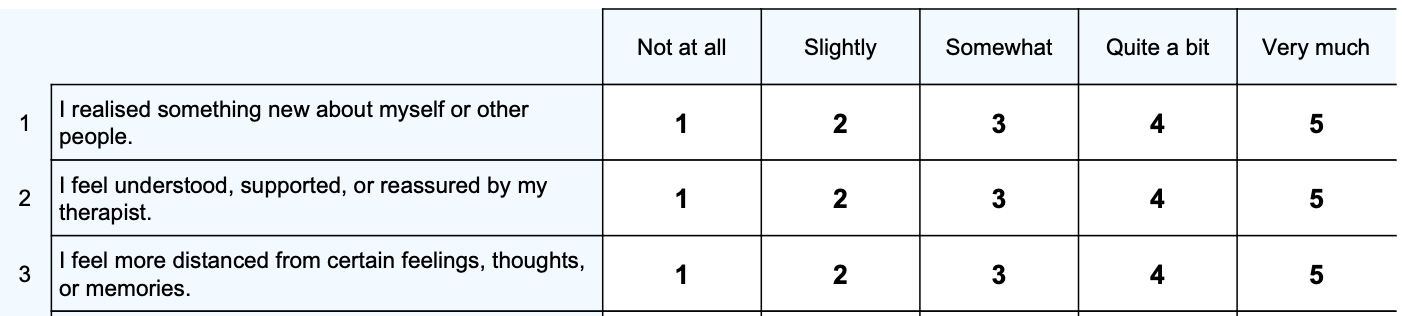
To conduct effective psychotherapy, understanding a clients’ perspectives is critical (Elliott & James, 1989) and clients’ experiences should be considered and addressed (Constantino et al., 2020; Wu & Levitt, 2020). However, some research suggests clients may not always be willing to honestly share their reactions to their therapeutic experience (Farber, 2020). Therefore, a concise method to encourage client feedback is crucial. The SRS-3-B is a brief assessment tool that can provide the clients’ perspective across two subscales:
The SRS-3-B can be meaningfully used both at the item level (yielding clients’ scores for specific reactions) and at the subscale level (yielding clients’ global evaluation of the session) with a higher score being indicative of more alignment with the question or subscale – therefore, a positive experience are typically indicated by higher Helpful Reactions score and a lower Hindering Reactions score.
It is important to note that higher scores on the Hinder Reactions subscale or lower scores on the Helpful Reactions subscale should be interpreted in light of a therapists knowledge of the therapeutic relationship. For example, this pattern of responding could be indicative of your client’s honesty with you due to their experience of unconditional positive regard. It is the process of using the SRS-3-B that is of greatest clinical use as opposed to just a simple interpretation of the score.
Raw scores and an average score (between 1 and 5) are presented. An average score for each subscale is presented so that the two can be compared (as there are a different number of items in each scale). The two subscales measured are:
For clinical utility, if there is significant variation/inconsistency within a subscale’s scores (defined as a standard deviation greater than or equal to 0.85), then a note is made in Interpretive Text that it might be better to be looking at the results of the SRS-3-B at an item level to gain better insight into the client’s view of the session.
A plot is presented after multiple administrations of the SRS-3-B so that you can track helpful and hindering reactions over time. When administered repeatedly, variations in patterns of responding are key to interpreting the results rather than absolute scores.
The original Session Reactions Scale-3 (SRS-3) was based on the Revised Session Reactions Scale (RSRS; Reeker et al., 1996), a brief self-report scale assessing clients’ immediate post-session reactions to their sessions, which itself is an extended version of the Session Impact Scale (SIS; Elliott & Wexler, 1994). To shorten the SRS-3 to the SRS-3-B, a combination of conceptual, empirical, and pragmatic criteria to select items was used with the purpose of still representing diverse types of reactions. Conceptual clusters were obtained from an expert sample as a basis for item selection, with the intention of retaining at least one item from each cluster. Empirically, the concurrent validity of the items was determined to see which items best represented established psychotherapy process constructs.
Exploratory factor analysis supported the use of the SRS-3-B as a two-factor (helpful reactions, hindering reactions) instrument (Řiháček et al., 2023). The SRS-3-B was meaningfully related to another process measure (Individual Therapy Process Questionnaire (ITPQ); Mander et al., 2015) both on the item and factor levels. The helpful- and hindering-reactions subscales, based on bolded items, had good to acceptable reliability (α= .88 and .77, respectively) and the two factors were relatively strongly negatively correlated (r = −.52). The helpful-reactions items had moderate to large positive correlations (.35 – .71) with the positive ITPQ subscales (i.e., in-session impact, confident collaboration, global alliance, and problem actuation); most also had small to medium negative correlations with the negative ITPQ subscales (i.e., patient fear and therapist interference). Items 2 (Understood, supported, or reassured), 7 (Clearer about problems/goals), and 11 (Personally invested) were most strongly related to the ITPQ global alliance subscale. Items 1, 4, 6, 9, 13, and 14 represent specific micro-outcomes and, as such, were well related to the ITPQ in-session impact subscale. Most hindering items had small to medium positive relations to the ITPQ patient fear and therapist interference subscales.