The BCEs scale also measures two primary dimensions of positive childhood experiences:
Example BCEs Items
For clinicians, the BCEs scale offers several distinct advantages, particularly in settings where understanding resilience factors is crucial for intervention planning. The measure is especially valuable for working with individuals who have experienced adversity, as it identifies existing strengths that can be leveraged in treatment. The BCEs scale can function as a strength-focused counterpart to adversity measures such as the Adverse Childhood Experiences (ACEs) scale, enabling a more balanced assessment of developmental influences.
The BCE offers clinicians a versatile tool for formulation, treatment planning, and therapy, particularly in trauma-focused settings. As a formulation tool, it can function as a strengths-based counterpart to adversity measures such as the Adverse Childhood Experiences (ACEs) scale, enabling a more balanced assessment of developmental influences. It can help clinicians identify protective factors in a client’s early life that may have buffered against adversity, while the absence of BCEs can highlight unmet needs that may have contributed to the formation of maladaptive beliefs or schemas.
In treatment planning, clients with few or no BCEs may benefit from a greater initial focus on establishing safety and trust in the therapeutic relationship before engaging in deeper trauma work. During therapy, understanding and exploring BCEs can foster hope and facilitates a strengths-based approach to meaning making and identity development. Additionally, BCEs can serve as existing strengths or resilience factors, which can be developed as internal resources for navigating trauma work in modalities such as EMDR and other trauma-focused therapies.
When using the BCEs scale in clinical practice, consider the following:
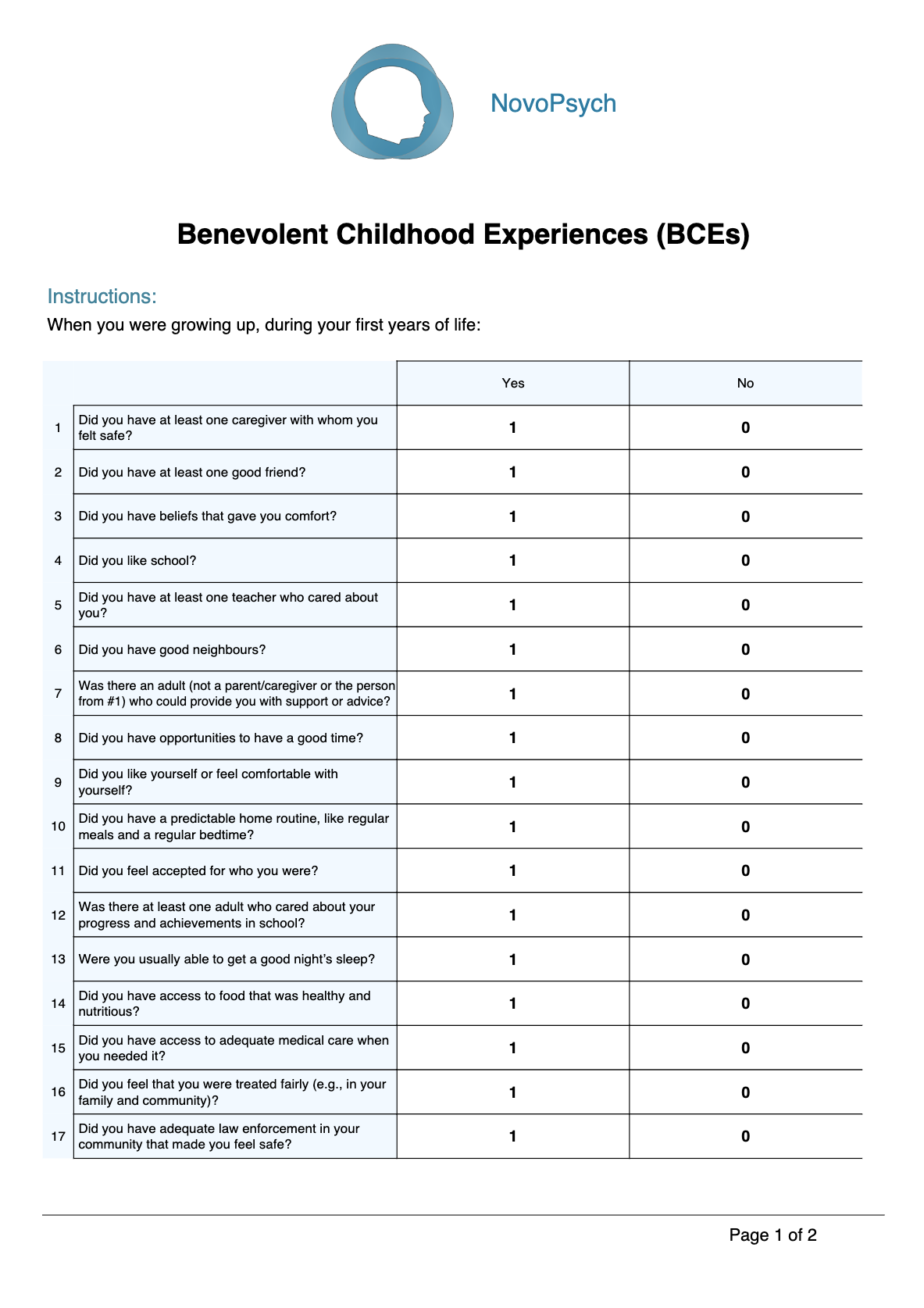
The BCEs uses a dichotomous (Yes/No) response format, with “Yes” responses summed to create total scores. The BCEs results in three scores:

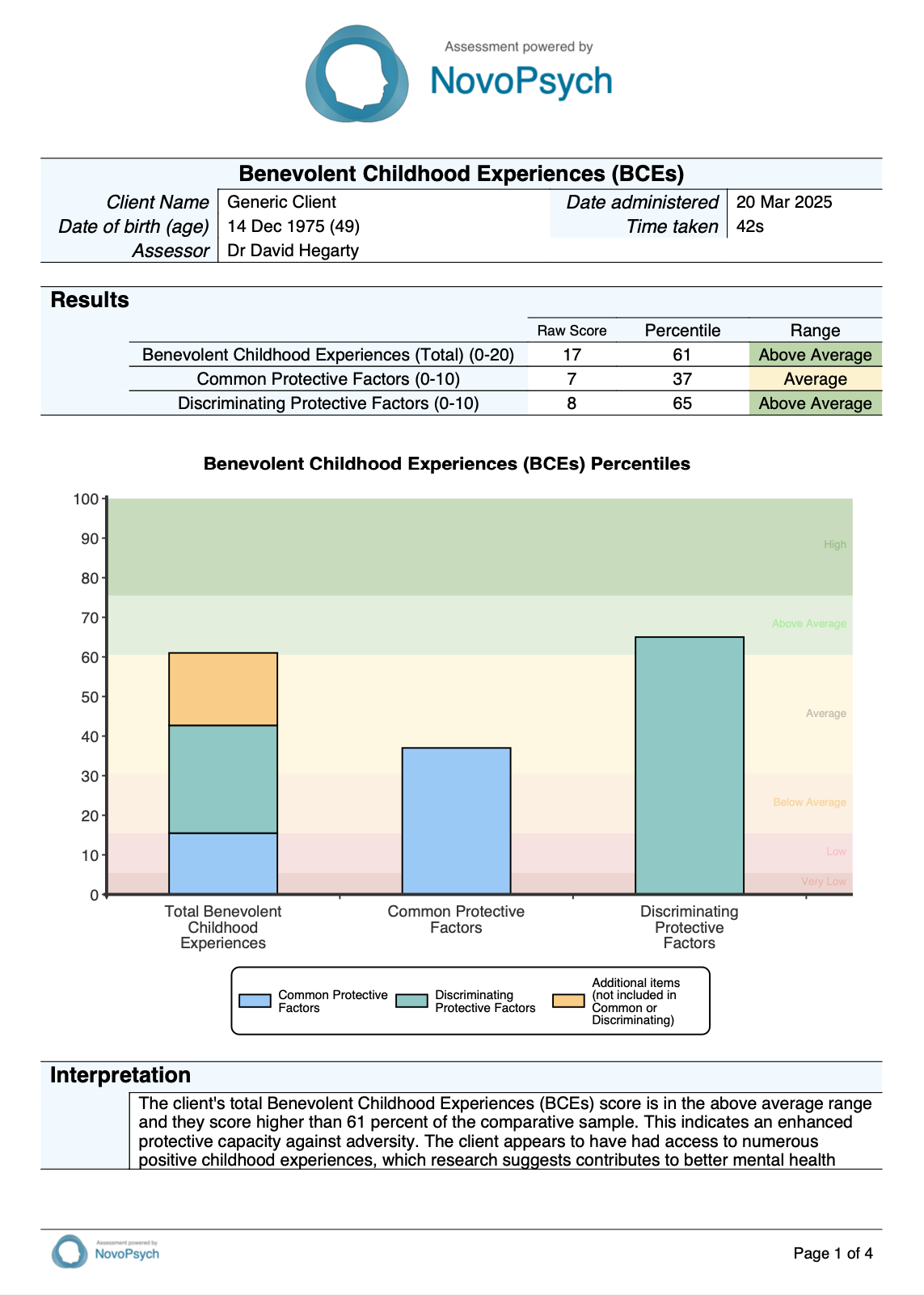
For each of these three dimensions, raw scores are converted to percentiles based on normative data derived from research with diverse populations. The percentiles provide a comparative framework for interpretation by indicating how an individual’s score compares to the reference population. A percentile of 50 indicates typical childhood experiences.
Qualitative descriptors are assigned to BCEs scores according to the following percentile thresholds:
These descriptors offer clinically meaningful categorisations that facilitate interpretation and communication of results. When interpreting BCE scores, consider the following clinical guidance:
Research indicates that each additional positive childhood experience is associated with incremental benefits to mental health and wellbeing.
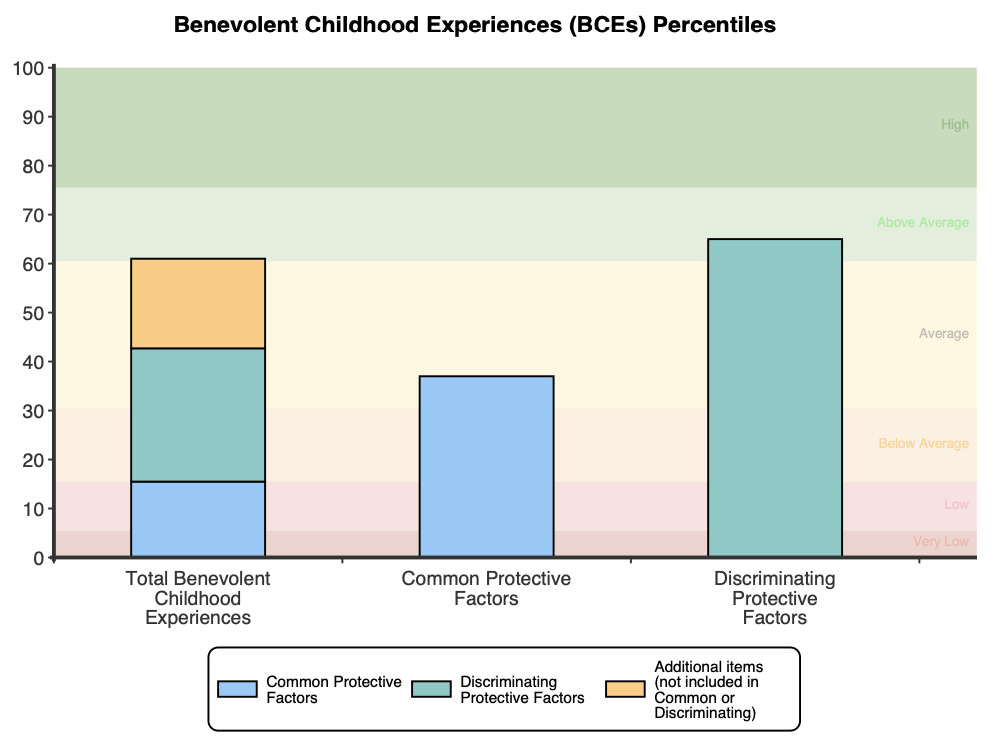
Upon first administration a plot is displayed showing the BCEs total score (made up of the common and discriminant protective factors and the six additional items that aren’t in either factor) and subscale percentiles. Qualitative descriptors are presented in the background of this plot for ease of translation. If administered on multiple occasions, an additional plot is presented showing the total score and subscale percentiles over time.
The BCEs scale contains 20 items but incorporates two different versions of the BCEs within those. Firstly, the BCEs-Original (common protective factors) which was developed by Narayan et al. (2018) and the BCEs-Revised (discriminating protective factors; Narayan et al., 2023) which was specifically developed to address ceiling effects in the original scale by focusing on less commonly reported positive experiences (those endorsed at rates below 80% across diverse samples). There are six remaining items that do not form part of either subscale but contribute to the total score on the BCEs.
Construct validity of the BCEs scale is supported by its ability to correlate with measures of wellbeing. The scale demonstrates expected inverse relationships with measures of depression, stress, and loneliness (Doom et al., 2021). Narayan et al. (2018) found that higher levels of BCEs predicted lower levels of PTSD symptoms and fewer stressful life events in pregnant women after accounting for women’s ACEs, and began to offset the effects of ACEs on negative outcomes even when ACEs were high.
Convergent validity has been established through correlations with other measures of resilience and positive experiences. The BCEs scale shows moderate to strong correlations with measures such as the Connor-Davidson Resilience Scale (r = .51) and the Protective Factors Survey (r = .63). Discriminant validity is supported by negative correlations with ACEs (Merrick et al., 2019), although these are only moderate in nature (r = -.33) indicating that they are not simply opposite ends of the same construct and that some individuals may experience high levels of both.
Cross-cultural validity is a notable strength of the BCEs scale. The initial psychometric study revealed that mean differences in total scores did not significantly differ between individuals who identified as White versus Black versus Latino/a, between individuals who were English-speaking or monolingual Spanish-speaking, nor between individuals who were born in the U.S. versus foreign born (Narayan et al., 2018).
Predictive validity has been demonstrated in multiple studies showing that BCEs scores predict mental health outcomes over time (Han et al., 2023; Narayan et al., 2018). For example, Doom et al. (2021) found that higher BCEs scores predicted lower levels of depression and anxiety symptoms during the COVID-19 pandemic, even after controlling for baseline mental health and demographic factors.
Normative data and percentiles for the BCEs total score were derived from item endorsement frequencies reported in research by Narayan et al. (2023), using data from two large samples of U.S. young adults (pre-pandemic sample, N=548, and pandemic sample, N=1,198). NovoPsych combined these using a weighted approach to create a statistically-derived normative reference population for the BCEs-20 total score. For the BCE-20, the estimated mean is 15.5 (SD = 5.38), for the common protective factors (BCE-Original) the mean is 7.72 (SD = 2.14; Narayan et al., 2023) and for the discriminating protective factors (BCE-Revised) the mean is 6.98 (SD = 2.70; Narayan et al., 2023). Raw scores are then converted to percentiles using a standard normal distribution transformation based on these estimated parameters. These percentiles are used to create qualitative descriptors as follows: