The scale includes six additional positive filler items (for a total of 44 items), with responses recorded on a 4-point scale ranging from 0 (never) to 3 (always).
The SCAS-Child measures six distinct anxiety dimensions:
For clinicians, the SCAS-Child offers several distinct advantages, particularly in both educational and clinical settings where understanding the specific nature of a child’s anxiety is crucial for intervention planning. Its comprehensive coverage of anxiety domains makes it particularly valuable for identifying specific areas of concern during initial assessment. Its alignment with diagnostic categories supports clinical decision-making and referral processes, while its ability to differentiate between various types of anxiety types facilitates treatment selection. The measure also enables tracking changes in specific symptom clusters over time, aiding in monitoring treatment effectiveness.
A parallel parent version (SCAS-Parent) is available, excluding the positive filler items but maintaining the same 38 anxiety-focused items. The availability of both child and parent versions enables clinicians to gather multiple perspectives on the child’s anxiety symptoms, enhancing diagnostic accuracy and treatment planning.
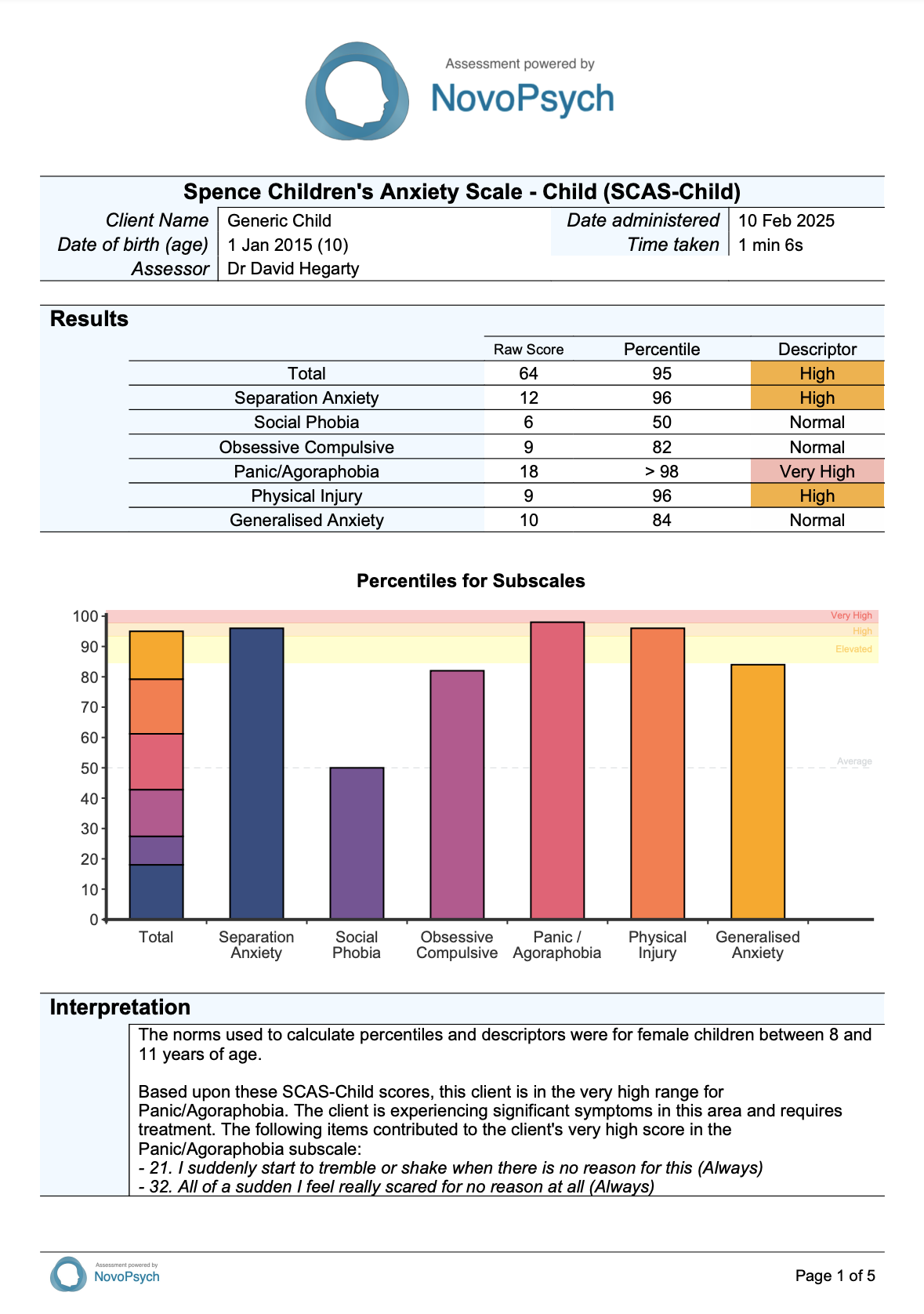
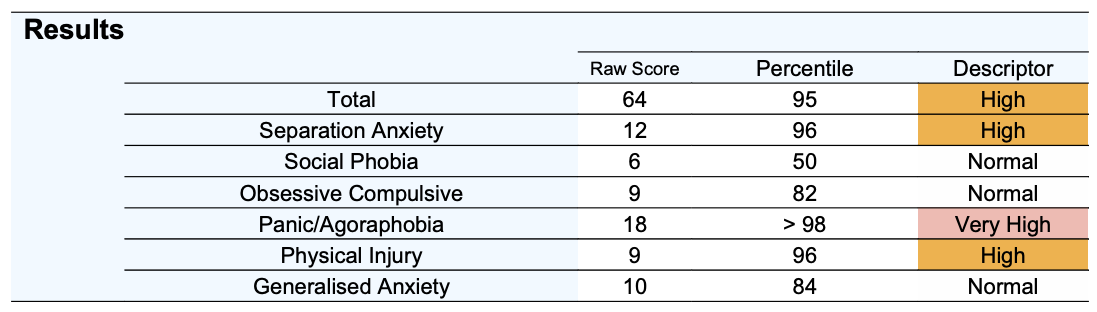
SCAS-Child scores consist of a total raw score (range from 0 to 114) and six sub-scale scores, with higher scores indicating greater severity of anxiety symptoms. These scores are also converted into percentiles based on age and gender from a large normative sample (N = 4,916) reported by Spence (n.d.) and accessible on www.scaswebsite.com. A percentile score of 85 and above for any subscale score or the total SCAS score indicates elevated and clinically relevant anxiety symptoms.
Sub-scales are presented for the SCAS-Child:
Items 11, 17, 26, 31, 38, 43, are positively worded filler items and are not scored in either the total score or the sub-scale scores, nor are items 45 and 46 which may elicit additional qualitative information.
A descriptor is determined that is based upon the percentiles:

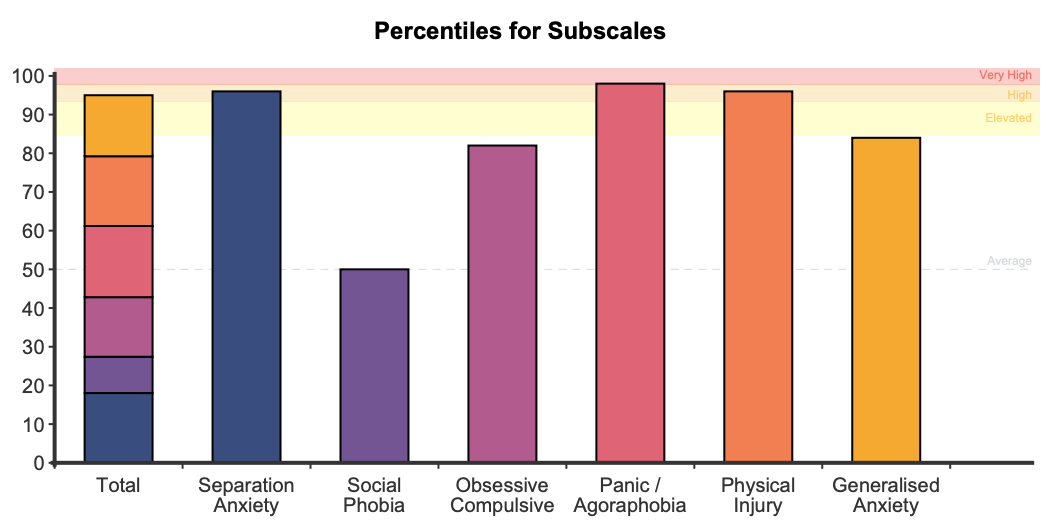
On first administration a stacked bar graph is presented showing the percentiles for the total score and subscales with the descriptors in the background of the plot. If the scale is administered on multiple occasions a graph is produced to track symptoms over time for both the total and the subscale percentiles.
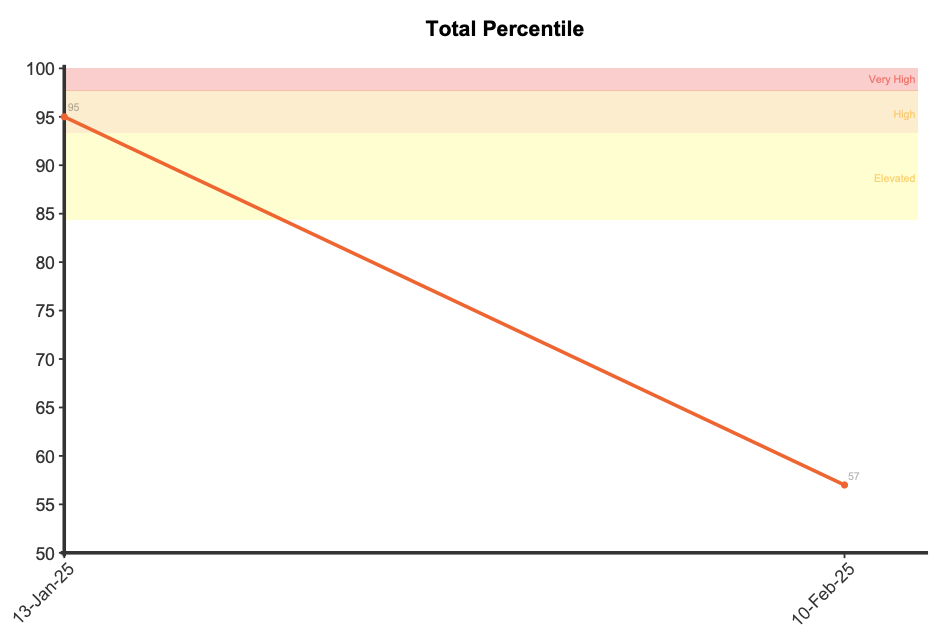
A reliable change score for the total score was determined by NovoPsych based upon 7,240 administrations of the SCAS-Child. The reliable change score was calculated as 14, meaning that if a client demonstrates a reduction of 14 points or more on the SCAS-Child total score then they have demonstrated significant improvement in their anxiety symptoms. Similarly, if they have demonstrated an increase of 14 points or more then this indicates a significant deterioration in their anxiety symptoms.
For comprehensive information visit the Spence Children’s Anxiety Scale website at: www.scaswebsite.com
The SCAS-Child has been extensively validated through numerous studies across multiple countries and cultures. Research has consistently demonstrated robust psychometric properties across clinical and community samples, with particularly strong evidence for its reliability and validity.
Internal consistency has been consistently high across studies, with coefficient alphas ranging from .87 to .94 for the total scale (Arendt et al., 2014; Delvecchio et al., 2015; Spence, 1998). The subscales show satisfactory to high reliability, with coefficient alphas typically ranging from .48 to .81. For example, Spence’s (1998) original validation study (N = 2,052) found internal consistency coefficients of .70 for Separation Anxiety, .70 for Social Phobia, .73 for OCD, .82 for Panic/Agoraphobia, .73 for Generalised Anxiety, and .60 for Physical Injury Fears.
Test-retest reliability has been examined across various time intervals, demonstrating good temporal stability. Spence (1998) found a 6-month test-retest reliability coefficient of .60 for the total score in a sample of 344 children aged 8-12 years. Subscale stability ranged from .45 (Panic-Agoraphobia) to .57 (Separation Anxiety and Social Phobia). Shorter interval studies have shown even stronger reliability, with coefficients ranging from .61 to .82 at 2-week intervals (Arendt et al., 2014).
The construct validity of the SCAS-Child is supported by its ability to discriminate between clinical and non-clinical populations. Spence (1998) demonstrated that children with comorbid social phobia and separation anxiety scored significantly higher across all factors compared to non-clinical controls. The scale shows particularly strong diagnostic accuracy, with Olofsdotter et al. (2016) finding significant predictive power (as measured by AUC) for both the total score and all subscales.
Convergent validity has been established through correlations with other well-established measures of child anxiety. The SCAS shows strong correlations with the Screen for Child Anxiety Related Emotional Disorders (SCARED; r = .85-.89), the Revised Children’s Manifest Anxiety Scale (RCMAS; r = .71), and the Multidimensional Anxiety Scale for Children (MASC; r = .71). Discriminant validity is supported by significantly lower correlations with measures of non-anxiety constructs, such as the Child Depression Inventory (CDI; r = .48) and the Strengths and Difficulties Questionnaire conduct problems scale (r = -.03 to .33).
The measure has demonstrated strong cross-cultural validity, having been translated into over 20 languages and validated across numerous countries including Australia, China, Belgium, Denmark, Italy, and the United States. A systematic review concluded that the SCAS is a reliable instrument suitable for cross-cultural use (Orgiles et al., 2016).
The SCAS Child Version has been validated in a large sample of Australian children (N = 4,916) by Spence (n.d.). This data is used to determine percentiles that are based upon age (8 – 11, 12 – 15 years of age, or combined (i.e., 8 – 15) if the client’s age is outside of these ranges) and gender (male, female, or combined if gender is not specified).
A descriptor is determined that is based upon the percentiles:
A reliable change score has been determined by NovoPsych for the SCAS-Child total score from data collected between July 2014 and December 2024 where clients had completed multiple assessments. All data was included in the analysis, so no data was removed based upon initial symptom severity. The resultant sample size was 7,240. The reliable change score was calculated using the Jacobson-Truax method of clinical significance classification (Jacobson & Truax, 1991) using a calculated Cronbach alpha from the NovoPsych data. The internal reliability calculated for the Total Score was 0.93 and the reliable change score calculated was 14.